
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Android | Pandora | iHeartRadio | TuneIn | RSS
A typical case of severe intraparenchymal hemorrhage with resulting herniation.
Takeaway lessons
- DOACs like apixaban (Eliquis), although not usually monitored using routine coagulation assays, tend to elevate the INR only slightly (e.g. 1.0–1.3 or so). A strikingly INR in warfarin-like ranges should raise suspicion for an additional occult cause of coagulopathy.
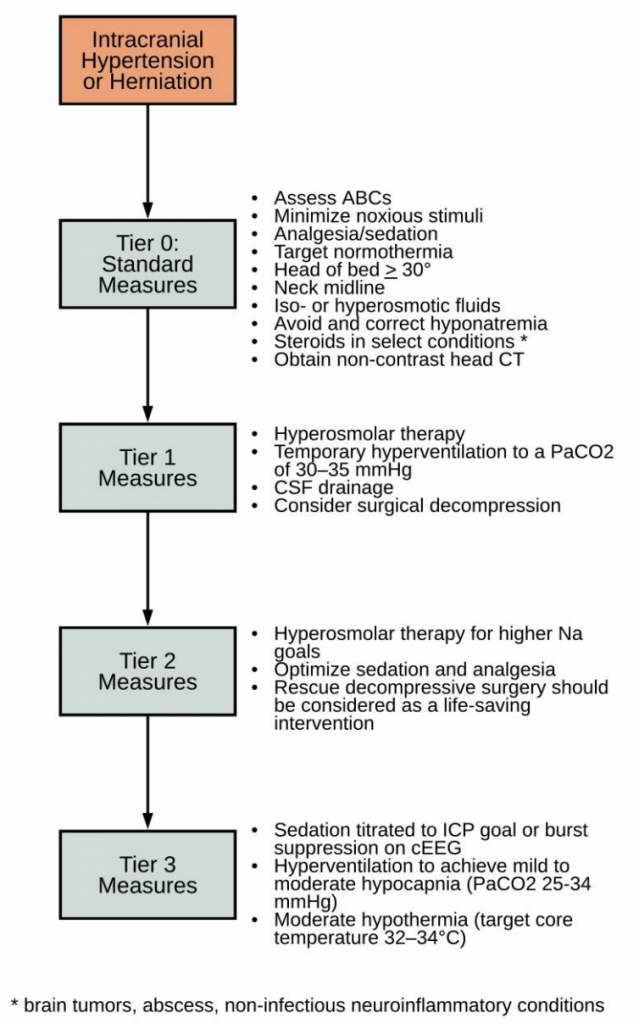
- Manage elevated ICPs using the ENLS “tiered” approach. All neurosurgical patients should receive the tier 0 (basic management) therapies.
- In the neuro-injured patient, seek “euboxia” to limit further brain injury: normal pH, normal PCO2, normal PaO2, normal BP, normal temperature etc.
- Be wary relying solely upon the GCS to describe, or even to trend neurological function. A descriptive, granular survey of function (particularly motor function) is usually more useful, as well as easier to remember.
References
Nestor MA, Boling B. Reversing Direct Oral Anticoagulants in Acute Intracranial Hemorrhage. Crit Care Nurse. 2019 39 (3): e1–e8.
Hi there! Just wanted to leave a quick note saying how much I love your podcast! Love the scenario based learning you provide. Solid information and knowledge and I think the best way to learn – give me a situation and then I can think through it and learn from the excellent guests you have on to work through it! Love it. Especially loved the flight scenario that was great.
Keep up the good work team!! Thanks for producing a great podcast!
~ Michelle Spresser RN CEN CFRN
Thanks Michelle!