Good sheath placement: ensure your skin nick is in the same hole as your dilator; use patient, steady pressure, especially as the “shoulder” (where the dilator meets the sheath) reaches the skin; insert the dilator completely into the sheath so you can see if it shifts, and dilate using both hands (one near the tip, one at the back holding the sheath and wire).
The right IJ is best (try to leave this open when placing non-positional lines like a triple lumen), left subclavian next best, third choice left IJ or right subclavian. Femoral placement is very tough without fluoroscopy; it requires two turns (into the RV, then out into the PA) and can be challenging to escape the RV. A brachial vein in the arm can occasionally be used as well.
Floating out of the left IJ is often obstructed by bumping into the innominate-SVC junction. Instilling just 0.5-1 cc of air in the balloon is often enough to float around this turn. This occurs less from the left subclavian or brachials, but if it does occur, the same maneuver may help.
Remember to place the contamination sleeve (Swandom) before inserting the Swan! Once you’re in, it’s too late; you’ll need to remove it and refloat. You don’t need to seal it, just get it around the catheter.
Flush each lumen before inserting and cap each one, except the distal/PA port. Connect that to your transducer and flick it to test transduction. Check the balloon; rarely, but sometimes, they will fail. Remember to always inflate the balloon using the included volume-limited syringe, and allow it to passively deflate from its elasticity.
If a balloon does not self-deflate, replace the catheter; the balloon is not reliable.
Once you reach 15 cm, inflate the balloon. By 15-20 cm, you should be in the RA; measure your RA pressure (overall mean is fine for ICU purposes). If the waveform is not distinct with clear components, flush the catheter; it may be damped by clots.
Tricuspid pathology (TR, stenosis) can make a Swan challenging, but not as often as people think. And the harder the Swan, often, the more important the data.
If you reach 30 cm without an RV tracing (except in some very large or very end-stage PH patients), you have probably gone astray, either coiled in the RA or gone through to the IVC.
Once in the RA, make a quarter rotation counter-clockwise (assuming you started with the tip curved medially). This will help orient the tip towards the tricuspid valve. If it’s not getting through, drop the balloon, come back to 20, readvance, repeat as needed.
If still not going, sometimes the tip has looped back into the RA while the middle of the catheter has “elbowed” through the tricuspid into the RV. If this happened, retract the catheter, and the tip may flop through as you come back. You’ll know this as the RV waveform will appear during retraction; inflate the balloon then and drive forward fast.
If you can’t get through a regurgitant valve, a faster/more aggressive advancement through the tricuspid valve may help. You need to launch through before it kicks you out.
Once you get an RV tracing, run! The faster you get through, the less likely you’ll have trouble. Most people who think they’re coiled in the RV are really coiled in the RA. The main exception is when the tip is pointed into the apex, and further advancement is just squishing you into that blind cul-de-sac. The other possibility is that you coiled in the RA, then the tip entered the RV; this usually manifests as difficulty wedging or reliably entering the PA, with all your slack in the RA. The only way out of these is to drop balloon and retract (to perhaps 35–45 cm), ideally not exiting the RV, but enough to change direction and readvance.
There should be a clear diastolic step-up as you enter the PA, with a change in diastolic shape (downsloping, not upsloping); there may or may not be a dicrotic notch.
Once you enter the PA, slow down. Advance a centimeter at a time. Wedge will usually occur around 50–51 cm; if you reach 55 cm without wedge, something has gone wrong.
Occasionally, the balloon size is inappropriate for the PA branch you’re in. Try deflating the balloon, then reinflate; you may find that it wedges before fully inflating (probably the catheter moved forward once you deflated it). You may also be in the wrong branch; come back to the main PA (around 45-50 cm), reinflate and readvance.
As you wedge, the pressure drop will be massive and obvious in pre-capillary/PAH disease; it may be less notable when PA pressures are elevated due to left heart disease. (Rarely the wedge may even be higher than the PA diastolic.) However, the waveform should significantly change.
If unsure if you’re fully wedged, drop balloon and readvance, see if it changes. When in doubt, draw a blood gas from the tip. The specimen should be arterial in oxygenation (eg SaO2 >92%). It is usually not needed to draw a simultaneous ABG peripherally to compare, and two simultaneous gasses may be easily mixed up in the lab. A “wedge gas” will have some resistance to aspirating the blood.
Once wedged and deflated, you can leave the catheter, or withdraw a little. If quite deep, maybe withdraw; the CXR will help guide you. The catheter will usually advance itself somewhat as it softens in the body, so if left quite deep it may auto-wedge later. If left too proximal, though, especially with high PA pressures, it may flop out of the PA. It is often necessary to leave a catheter in a spot where it needs to be floated forward a couple centimeters each time you want to rewedge, which is fine.
Once left in the body for a while (~30 minutes), it is nearly impossible to readvance into the PA (if it escapes) due to increased catheter floppiness.
Daily CXRs are still the standard in patients with a Swan to monitor for tip migration.
All measurements are ideally taken at end expiration, but for bedside purposes, this is often not too important; the mean monitor number may be adequate.
The best way to avoid PA injury during wedging is to check your tip position and ensure it’s not too deep or auto-wedged before you inflate. Remember that you don’t need a full syringe to wedge everyone; once you wedge, stop inflating. Use good communication with your team during insertion, to ensure the balloon is down and the catheter position locked when you leave it.
An overwedged waveform will show continuously rising pressures, often very high (either it’s too deep or turned into the wall). Deflate and retract. If your wedge keeps rising as you measure it, you’re probably overwedging.
A TTE view of the RV base/RVOT view (parasternal or subcostal – latter may even be better) might be helpful for guidance in the absence of fluoroscopy, as you’ll see the tricuspid valve, RV, and pulmonic valve.
Tricuspid valve issues are the most important relative contraindications for a Swan without guidance, particularly an artificial valve or tricuspid endocarditis.
If you don’t need to monitor PA pressures/wedge, probably remove the Swan; you can leave the sheath if you think you might want to measure later. Retracting it to an RA position will probably not leave the possibility of refloating later, as it will be all floppy by then; just remove it and float a new one later if needed.
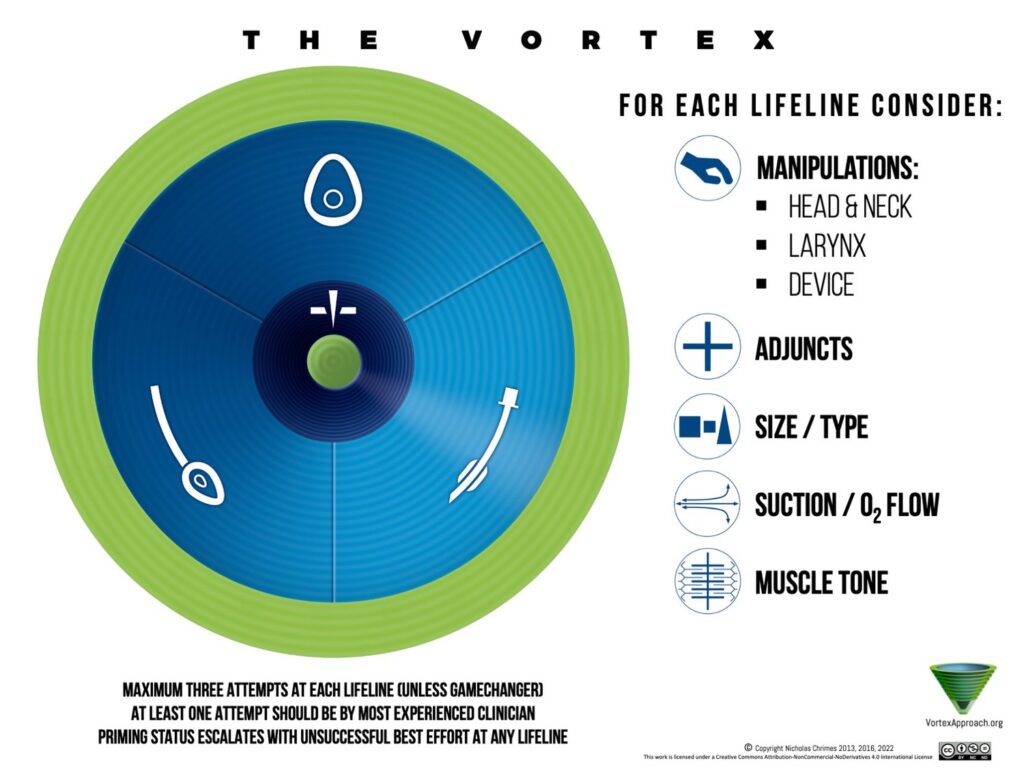
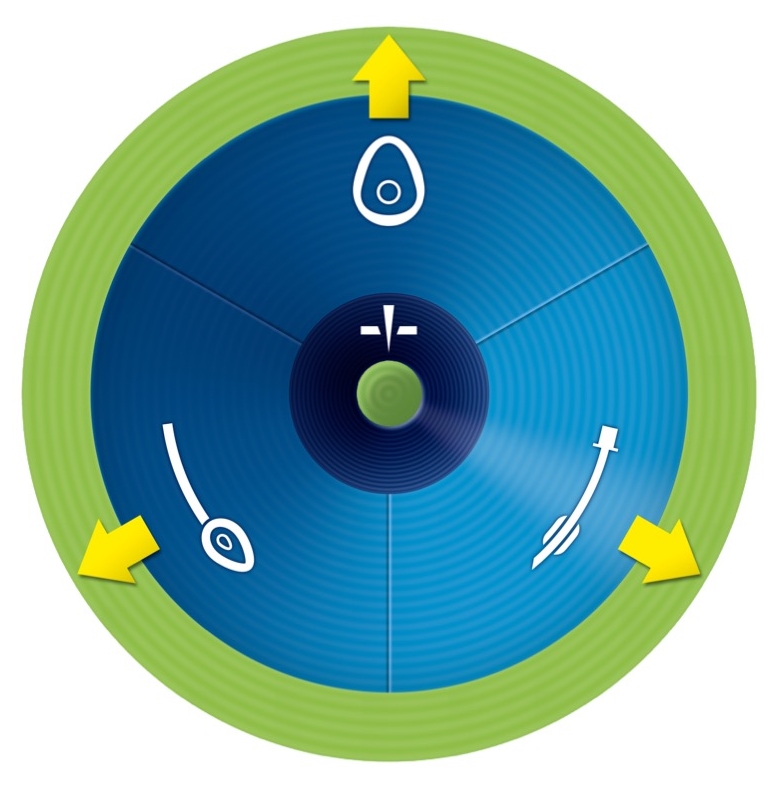
We learn about the Vortex approach to airway management, as well as airway algorithms and mental models in general, with Vortex creator and anesthesiologist Dr. Nicholas Chrimes, anaesthetist and cofounder of the Safe Airway Society.
We discuss the basics of evaluation for tracheostomy placement, periprocedural care, and post-procedure complications with Vinciya Pandian, PhD, ACNP, FCCM, tracheostomy nurse practitioner and researcher.
We discuss assessment, monitoring, medical stabilization, and when to consider transplant of the patient with acute liver failure. We are joined by Dr. Sergio Navarrete, anesthesiologist and intensivist with fellowship training in transplant anesthesia.
Transaminases rising into the many hundreds or thousands (especially with pre-existing liver disease), or a MELD in the low teens (from baseline normal) should raise concern for a concerning degree of liver injury, usually due to shock liver, congestion, or infection. This should also prompt consideration for transplant evaluation, and usually a phone call to your transplant center.
Reversible causes, such as acetaminophen toxicity or portal vein thrombosis, must be ruled out.
Optimization of perfusion should include not only the left-sided systemic circulation, but also the right-sided system and venous congestion; congestive hepatopathy (from volume overload or RV failure) can absolutely cause severe liver injury. Echo, potentially with tools like VEXUS scoring, can be a great help here.
N-acetylcysteine has a clear indication for treating acetaminophen poisoning, but not much data for other causes of liver failure. However, many clinicians believe it may provide some benefit, and there is probably no harm—other than administering a fair amount of volume.
Hypoglycemia and hypothermia are both relatively late and ominous findings in the ALF patient (put them on a dextrose infusion and hourly glucose checks). Transaminase levels reflect hepatocyte injury but not liver function. Synthetic function as measured by INR or fibrinogen are helpful. Bilirubin is usually too slow and non-specific to be actionable. Trend this stuff every 6 hours or so.
Mental status is a key monitoring tool as a marker of cerebral edema. The clinical exam, ammonia level, potentially serial CT scans, and maybe invasive ICP monitoring (Sergio prefers a bolt over EVD) may all be needed in high-risk cases.
The highest risk patients for cerebral edema are those with truly acute/hyperacute liver failure. Trend ammonia, which has some correlation with herniation risk, but the neuro exam is more useful. Neurosonography could be used as well.
Lactulose should be used, and in extremis hyperosmolar therapy considered, although data for this is less clear than in other neurologic emergencies.
Liver ischemia and death will reliably cause a systemic inflammatory state with resulting distributive shock; this can persist even after transplant, due to persistent elements of the dying liver. Treat this like any SIRS/distributive shock state.
Bleeding and clotting can both occur; numbers usually suggest coagulopathy, but hemostatic rebalancing is often present, at least until something perturbs the balance (e.g. a procedure). Labs like the INR are a marker of disease severity, not bleeding risk. Fibrinogen is a little better, but TEG is probably the most useful marker of bleeding status, as many of these people are actually hypercoagulable.
Some would use CRRT relatively early in a liver failure patient; Sergio would not. However, he would consider it in the volume overloaded patient to manage congestion (if diuresis proved inadequate).
Liver-specific extracorporeal organ support using various devices (MARS, “liver dialysis,” albumin dialysis, etc) are interesting/promising therapies that largely have not shown convincing benefit in studies. They tend to be sporadically available and highly institution-specific.
In all cases, earlier consultation to liver transplant specialists is better than later (this may involve an interfacility phone call or transfer). Several days are usually needed for transplant evaluation, many aspects of which are not directly medical, such as assessment of social support, insurance, pre-transplant workup, etc. Waiting too long may mean a patient dies before the process can be completed.
All truly acute liver failure should be referred for transplant evaluation.
Typical rule-outs for transplant include uncontrolled metastatic malignancy, age (often >75; every center has a different cutoff), and severe unrepairable cardiac dysfunction. Infections such as active bacteremia are a concern. Much of this is a judgment call and up to the transplant team, and their culture and policies.
Alcohol use is not necessarily a rule-out for transplant; some (not all) centers will consider these patients. The social milieu is more important. It is not unreasonable to refer a patient to a more distant center that has broader eligibility criteria than a nearer one that rules them out.
Some critically ill patients may be transplant candidates, particularly if most of their problems are deemed secondary to their liver failure and hence potentially reversible. Liver transplant is a procedure that can and often should be performed in the setting of multi-organ failure, shock, respiratory failure, etc. But each center has its own risk tolerance.
In any sudden loss of pulse/consciousness, particularly in a known cardiac patient, the presumption should be for a shockable arrhythmia and rapid defibrillation should be prioritized above all else.
Anterior-posterior pad placement may or may not be superior, but tends to be logistically helpful, as it allows rolling the patient a single time then never again; a second set of pads can be added for double sequential defibrillation without moving them, and a mechanical compression device can be applied at the same time as the pads.
The primary or highest-trained provider should not be the sole “code runner,” but ideally offering high-level leadership, thinking about reversible causes and judgment calls, and performing procedures, while another leader (often a nurse) runs the standard activities of ACLS such as timing, coordinating rhythm checks, assigning jobs, quality assurance, and directing the room. That frees your cognitive bandwidth by handling all your logistics, and they can act as the one-stop-shop for passing needs and issues up and down the chain.
IOs are probably the go-to for immediate access, if no IVs are present. But Scott likes to always place central access, usually femoral. He does ECPR, so the access may be needed, and even if not, it maintains the skill for next time. He also likes an arterial line, so it’s easy to place venous alongside it. He would generally not place it fully sterile (gowns, drapes, etc), but will use sterile gloves and prep the skin, assuming that any femoral line placed in the ED is going to be replaced within 24 hours.
Scott loves an arterial line. It eliminates the “pulse check,” allowing instant confirmation of pulsatility, while also allowing a very sophisticated assessment of coronary perfusion.
A diastolic BP above 35–40 mmHg, measured from the arterial line during cardiac arrest, suggests adequate coronary perfusion. This must be measured manually, as the automated number will falsely measure the wrong spot in the waveform during the “suction” of chest recoil (see link below); the true point of measurement is just before the upstroke of systole begins. If you’re above this DBP, just skip epinephrine, which will probably merely be toxic (ie promoting arrhythmias).
A low DBP should be used as a general marker of poor perfusion, and prompt other changes. Try modifying the point of compressions on the chest to avoid obstructing the LVOT (TEE is even better for this, but not available most places). Swap out compressors to ensure the most vigorous compressions, even if they still “look okay” or claim to be. Look for a reversible cause, such as hemorrhage or obstruction. Finally, if it’s truly just vasoplegia, consider other moves, such as adding vasopressin/steroids (an evidence-based practice) or high-dose epinephrine (5 mg epinephrine).
ETCO2 should be used in all arrests, to confirm airways, prognosticate, and provide a marker of perfusion much like the arterial DBP.
Scott thinks we should stick to 30:20 mask ventilation when an airway is not in place; breaths don’t really go in during compressions, and bagging during the upstroke is very tough. But he prefers to just insert a supraglottic airway quickly and use that, a skill anyone attending cardiac arrests should have. If using the BVM, you should use capnography to confirm breaths are actually going in.
Intubation should be done with video if available. Hyperangulated or regular geometry are both fine. Use a bougie if you have regular geometry (and are good with it). There should never be an intentional pause in compressions for the airway, however; just intubate during compressions, not so hard with video and a bougie. Position the patient optimally, just as in any situation; don’t rush.
Never perform “pulse checks,” only rhythm checks. If the rhythm is non-perfusing, resume compressions. If it’s organized and potentially perfusing, only then check for a pulse (or preferably your arterial line).
POCUS is essential: look for pericardial effusions, a dilated RV (although this is usually present), signs of hemorrhage, and pneumothorax. Maybe even more importantly, use it for pulse checks rather than your fingers. Scott will start with this, and if a “sonographic pulse” (visual pulsatility of the vessel) is found, he’ll then apply his fingers to see if it’s strong enough to feel. At this moment in time, he thinks palpability is a reasonable cutoff for when to call flow PEA vs hypotension.
Once he’s ruled out reversible causes, he tries not to look at the heart with ultrasound, since it tends to detract from compressions (without TEE); sonographic pulse implies organized cardiac activity. An arterial line obviates all of this, although it’s not clear what BP is adequate; Scott still uses a DBP 35-40 but would accept a MAP of 40 as a reason to defer compressions, if rapid efforts are undertaken to increase it.
Scott always likes mechanical compression devices when available (he likes the Lucas), which ensures good quality, provides a backboard, and reduces the energy in the room, even if it doesn’t improve outcomes. Buy one for your hospital’s code team and bring it to the arrests. If not available, he likes a backboard.
The impedence threshold device (ITD), potentially in combination with active compression-decompression devices, is interesting but the initial promising data has not been replicated; he would not consider this ready for use.
Heads-up CPR is also interesting but not yet proven.
When defibrillating, always max out the current on the machine. It creates no meaningful injury and maximizes your chance of conversion.
When a shockable rhythm is seen, he resumes compressions while charging, and in fact often performs hands-on defibrillation (shocking during compressions, using some kind of standoff between hands and chest, such as a towel, or even just gloves); mechanical compressions make this easiest.
Pre-charging before the rhythm check is wise, and the nurse code leader can coordinate this; do it every time.
Amiodarone or lidocaine are equally reasonable first line antiarrhythmics. If they’ve had one and you’re still in electrical storm, try the other.
If storm persists, these are excellent ECPR cases. Otherwise, you can try esmolol (bolus 500 mcg, usually no drip), then double sequential defibrillation.
DSD: don’t let pads touch; shock as simultaneously as possible (used to be intentionally separated, but some data now suggests closer together is better). There is a very small but real risk of damaging defibrillators doing this (and the damage may actually not be obvious, i.e. the machine will still pass a later self-check).
How long to go? Depends on baseline functional status, rhythms seen, and other factors. Past 40 minutes of low-flow time, arrest is probably not survivable without ECPR (for which the cutoff is probably 90 minutes), unless there has been stuttering flow (intermittent ROSC), which tends to reset that timer. ETCO2 persistently <10 is very poor. No cardiac motion seen on echo in PEA is poor.
One exception might be if your interventional cardiologists are willing to cath intra-arrest during mechanical compressions; in that case you might go longer to bridge to this.
In a young or baseline well patient, Scott would almost never stop before 40–45 minutes.
Scott always runs a norepinephrine drip at 50 mcg during the arrest, making it easy to transition to the drip after ROSC and avoiding any delays.
After ROSC, a STEMI or high-risk patient should go to the cath lab. Everyone else should have a pan-CT, including head, chest, abdomen/pelvis. This ideally is gated/timed to triple rule out PE, coronary occlusion, and aortic dissection. It also identifies important post-CPR trauma.
In 2025, Scott’s take on TTM is reactive: place an invasive temp probe (esophageal or Foley, not rectal, which is too slow and inaccurate) and monitor for fever; if it occurs, then cool actively to normothermia. There are probably some patients who benefit from more cooling, but nobody knows who (longer downtimes?). This method is as good and cheaper than empirically applying a cooling device to maintain normothermia before fever occurs, and that might cause problems, such as if it aggressively cools for a trivially increased temperature and induces shivering. Put the cooling device at the bedside without opening the pads if you really want to be ready.
If having trouble inserting your floppy esophageal temp probe, use an esophageal stethoscope from the OR, or use a split 8.0 ET tube to introduce a lubricated probe into the esophagus.
For out-of-unit codes, it’s all the more important to have a nurse code leader. A code team should bring the specialized equipment (maybe make a cart) to the bedside, such as mechanical compression devices, ultrasound, capnography, etc.
We talk about the phenomenon of airway closure during mechanical ventilation, with Thomas Piraino, RRT, FCSRT, FAARC, adjunct lecturer for the Department of Anesthesia at McMaster University, editor of The Centre of Excellence in Mechanical Ventilation Blog, and a member of the editorial board of Respiratory Care.
Airway closure occurs when airways, probably smaller ones (ie bronchioles) completely collapse at some point during expiration, causing flow to cease.
This creates a false understanding of the “PEEP,” which may actually be higher than the set PEEP (effectively an autoPEEP), and hence an incorrect understanding of the driving pressure and compliance. (This autoPEEP may or may not be effective, as at higher FiO2s, this trapped volume may rapidly absorp, causing absorption atelectasis.)
It may cause lung injury at the airway level from cyclic opening/closing, separate from more-discussed alveolar injury.
ARDS, pulmonary edema, and obesity are all risk factors. Post-cardiac arrest is a particularly common substrate. Obstructive diseases like asthma/COPD can probably see this as well, although the recent discourse has focused on the hypoxic conditions; the phenotype is probably different, caused by intrathoracic pressure, not by air-fluid interfaces and surfactant issues.
Probably 40% of at-risk patients may see this phenomenon occur. Its presence and the pressure where it occurs may be labile and dependent on the clinical condition. It should probably be checked at least daily in such patients.
It may cause hypercarbia by terminating expiration early, leading to air trapping. Prolonging the expiratory time will not help, as flow has ceased.
Plateau pressure may be elevated. Expiratory holds will not reveal this, however. A visible inflection point in continuous-flow VC breaths that has a different height (higher) than the gap between the peak and plateau pressure may be a rough suggestion of this as well.
Plateau pressures will be accurate, as the airways should be open at peak inspiration (or no breath would be delivered). Thus, increasing PEEP and seeing no change in plateau pressure may be a sign of airway closure, although it can also be due to alveolar recruitment.
Active patient effort during exhalation may worsen this phenomenon, particularly in the obstructive patient, due to increasing intrathoracic pressure.
The best test is a slow-flow inflation curve. Draeger and Hamilton should have this built in (Hamilton does this incrementally, not continuously, which may make it a little harder to identify the exact inflection point). It can be done manually as such (patient must be passive):
Set VC mode
Square wave flow
Flow 5L/min
Rate 5/min
PEEP 5 (or higher if needed for oxygenation)
Freeze the screen and inspect the pressure scalar during inspiration. The upramp should be steady and continuous. If there is a change in slope or inflection point, this suggests a change in compliance, probably due to airway opening. Use the vent to measure pressure at this point.
A clever time to do this might be shortly after intubation, while patients are deeply sedated and paralyzed.
That this inflection represents airway opening can be proven by measuring the compliance up to that point (volume delivered vs pressure), which will usually be <3 cmH2O/ml, roughly the compliance of the ventilator circuit.
Inflection can occur from alveolar recruitment as well, but this is usually a less abrupt, steady change in slope. If present, it will occur above the airway closing pressure inflection.
In general, set the vent PEEP at the same level as the measured closing pressure. This will normalize your understanding of the driving pressure and probably limit cyclic collapse and lung injury. It may also facilitate expiration and hence ventilation.