Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Android | Pandora | iHeartRadio | TuneIn | RSS
A brief discussion of the stuff in your pockets as you practice medicine.
Educational critical care scenarios presented in a podcast format.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Android | Pandora | iHeartRadio | TuneIn | RSS
A brief discussion of the stuff in your pockets as you practice medicine.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Android | Pandora | iHeartRadio | TuneIn | RSS

We discuss the nuts and bolts of urinary infection with an obstructing stone with Ashley Winter (@AshleyGWinter), board certified urologist with a fellowship in male and female sexual medicine, and chief medical officer of Odela Health.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Android | Pandora | iHeartRadio | TuneIn | RSS
From the Critical Concepts blog, thoughts on our personal biases and lack of humility when contemplating end-of-life decision making.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Android | Pandora | iHeartRadio | TuneIn | RSS
Bryan and Brandon chat about holding down jobs, conflict resolution and interpersonal skills, and how to protect yourself as an employee.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Android | Pandora | iHeartRadio | TuneIn | RSS
When are patient outcomes your fault?
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Android | Pandora | iHeartRadio | TuneIn | RSS
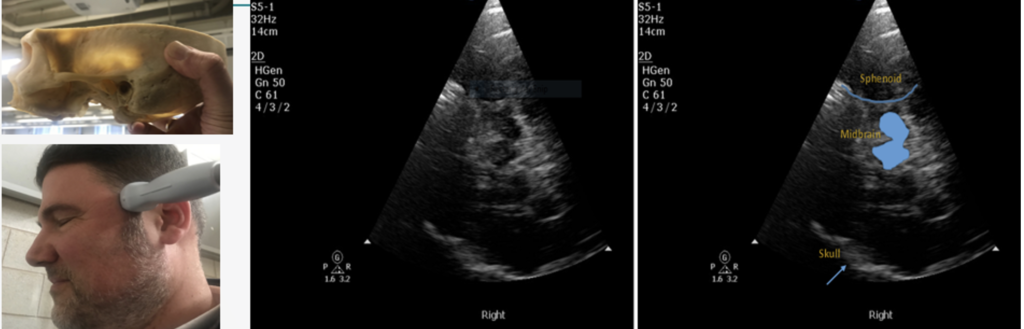
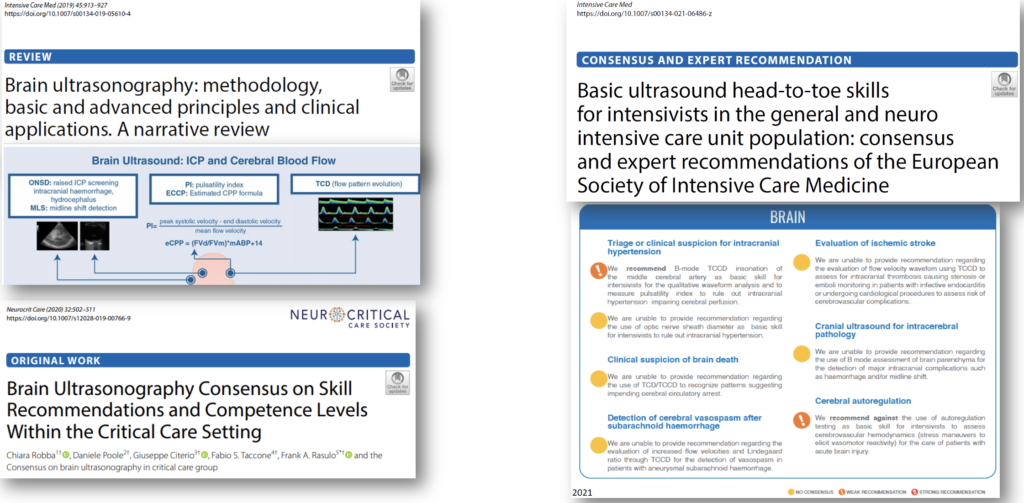
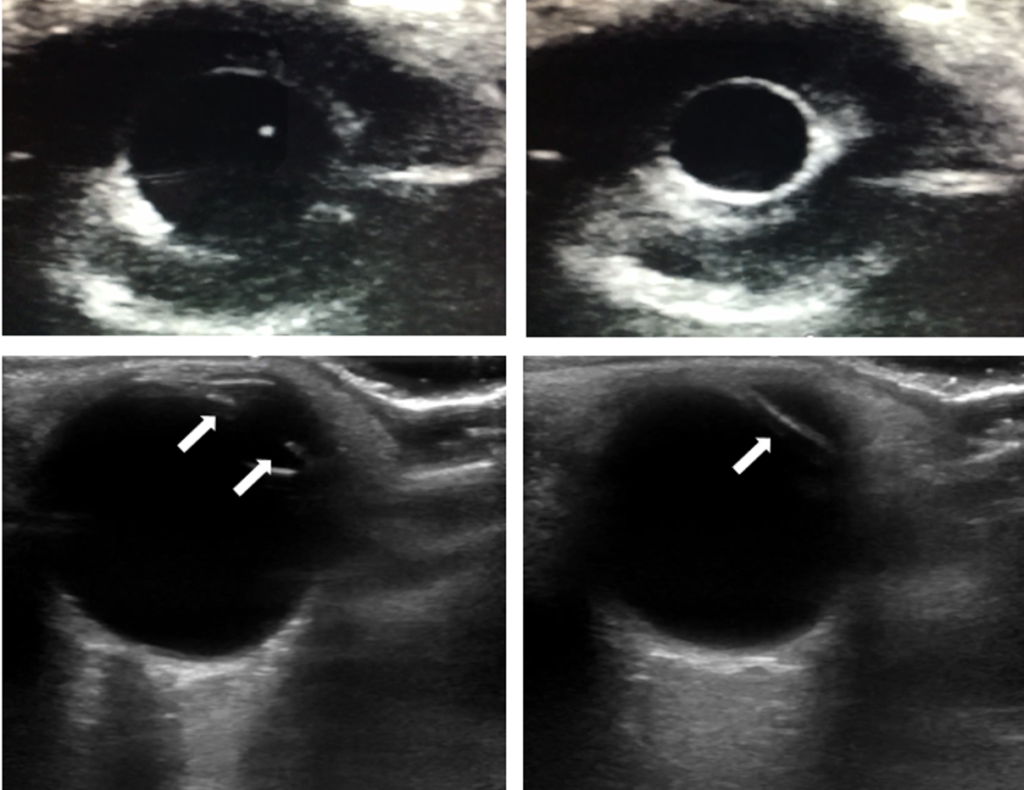
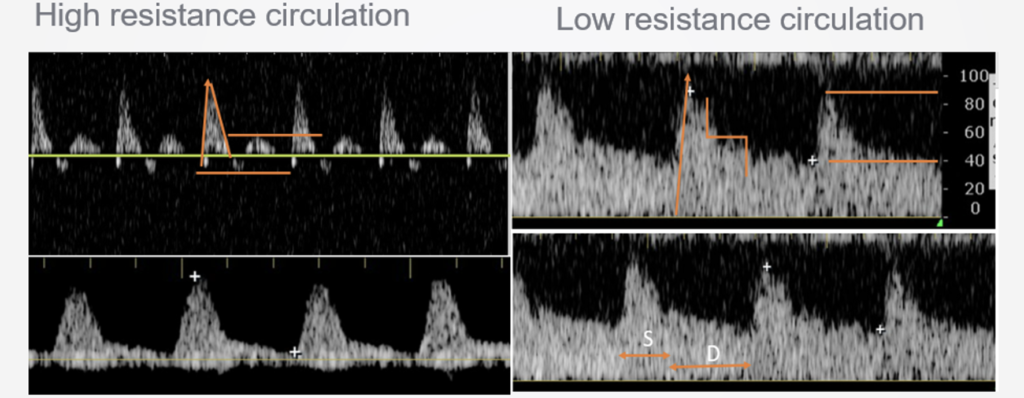
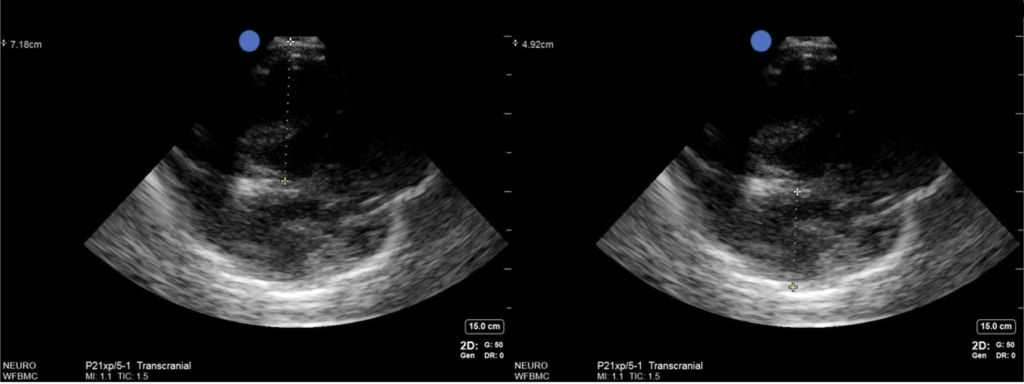
We explore the cutting edge practice of point-of-care ultrasound of the brain, including optic nerve sheath measurement, transcranial doppler, assessing midline shift, and more, with Aarti Sarwal, neurologist and neurointensivist, director of the neurocritical care unit at Wake Forest, and director of their neurovascular lab and ultrasound courses.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Android | Pandora | iHeartRadio | TuneIn | RSS
Dealing with the good and bad aspects of tissue mobility during percutaneous procedures.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Android | Pandora | iHeartRadio | TuneIn | RSS
We chat with friend of the podcast Matt Siuba (@msiuba), Mr. Zentensivist, to share our distinct perspectives on the relationship between APPs (PAs or NPs) and the intensivists we work alongside.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Android | Pandora | iHeartRadio | TuneIn | RSS
The dilemma of lung-protective ventilation in patients with strong spontaneous breathing.
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | Spotify | Android | Pandora | iHeartRadio | TuneIn | RSS
We dive into when to initiate renal replacement therapy, the modalities, settings, and physics involved, troubleshooting problems, and more, with Dr. Paul Adams, a dual-trained nephrologist and intensivist at the University of Kentucky.