We chat about managing a complex MICU patient with RV failure in the setting of renal failure and sepsis, with Amos Dodi, nocturnal intensivist at Einstein/Montefiore and author of a recent narrative review on the RV.
Distinguishing the cause of shock in a patient with chronic PH is always challenging. Echo can be harder to interpret, but extremes can be called: frank hypovolemia, frank RV failure. Don’t forget to correlate clinically, eg feeling the extremities to estimate SVR.
Measuring CVP can be very valuable in these patients. The spot value can be hard to interpret, but trends can be revealing; if the CVP suddenly jumps, consider the RV is giving up.
Response to therapy can also be a potent diagnostic tool, such as the response to inotropy, or a fluid challenge.
Avoid hypoxemia, hypercarbia, hypotension, acidosis, all of which increase the PVR and hence RV strain. Limit fluid inputs from drips.
Favor vasopressin as a PVR-sparing pressor, perhaps with low-dose epinephrine as a titratable inopressor, though caution with vaso causing coronary ischemia in an RV already at risk of it due to dilation.
Intubating the RV failure patient should be done with great caution and respect, and really, deferred if possible. The team should proceed with awareness of the risk of hemodynamic decompensation (ideally one provider tasked to this purpose peri-intubation). Induction agents should be hemodynamically stable, preoxygenation should be optimal, and be delicate with BVM use to limit intrathoracic pressure.
A PA catheter has potential utility, although expertise has dwindled these days. It is not impossible that placing a foreign body across the TV, through the RV into the PAs could even worsen RV function somewhat. Non-invasive cardiac output monitors may have a role as well although the benefit has not be clearly shown.
Volume management and diuresis can sometimes be guided by the urine sodium.
We dive into the confusing rabbit hole of medical staffing, credentialing, and privileging, particularly for the critical care APP, with Chris Newman, pediatric critical care PA and Vice Chair for Clinical Performance at the University of Colorado.
The medical staff office regulates the medical staff, which includes physicians and APPs. The latter may actually be voiting “members” of the medical stuff, or have some kind of affiliate status; the relevance of this is their eligibility to vote and sit on its committees, which sets the policies and manages governance. Either way though, APPs are subject to the medical staff office’s regulation.
Credentialing is the process of ensuring medical staff have the right and competence to work in the hospital, mostly confirming basic job requirements like graduating training programs. Privileging is the process of determining what specific things you are allowed to do in the hospital.
Privileges are broken into core privileges, which are things any provider should know how to do (i.e. taught in school): perform H&Ps, order meds and tests, interpret them, etc. Special privileges are those that require additional training, usually procedures. Some of the latter may become core privileges over time.
Special privileges are needed for anything “infrequent and high risk,” which requires some judgment – i.e. if a procedure is not listed, does that mean you cannot do it, or that it does not even require special privileges? Which procedures are listed is determined by the judgment of the clinicians in medical staffing, and the list is not always perfect.
All of these processes are hospital based, usually not part of state law, and are also often subject to Joint Commission regulation. However your hospital handles them, it is expected to follow its own policies consistently.
Learners are managed under policies for proctoring, not privileges. A person with procedural privileges can generally supervise a learner without privileges to perform it; if that’s a student, it is considered to be “done” by the proctor, and if by a licensed provider without privileges, it is “done” by the learner under supervision. Such a learner may eventually obtain their own privileges (usually by meeting a requirement of either numbers or observed competence or both). The exact rules of how all this works is governed by a proctoring policy which can be looked up.
While many providers may feel it is accepted, or even an ethical obligation, to perform procedures they are trained but not privileged to perform in an emergency (i.e. to save a life when a privileged person is not immediately available), there is usually no explicit allowance for this in hospital policy, so buyer beware.
If you don’t like how your processes work, change them.
We discuss the practicalities of running a rapid response, including crowd management, coordinating with primary services, working outside the ICU, and rapidly obtaining and synthesizing diagnostic data.
We explore the practical intricacies of nebulized medications, including timing, dosing, types of devices, and more, with Keith Lamb (@kdlamb1), RRT, RRT-ACCS, FAARC, FCCM.
We explore the practical basics of managing an elevated ICP with impending herniation, including EVD troubleshooting, hyperosmolar therapies, and the role of craniectomy.
With Dr. Prem Kandiah, neurointensivist, transplant intensivist, and ammonia enthusiast, we explore the physiology of hyperammonemia, the nuances of its measurement and interpretation, and unpack some less-recognized causes, including infection by urease-producing organisms and malnutrition/gastric bypass.
Bernal, W. and J. Wendon, Acute liver failure. N Engl J Med, 2014. 370(12): p. 1170-1.
Bernal, W., et al., Lessons from look-back in acute liver failure? A single centre experience of 3300 patients. J Hepatol, 2013. 59(1): p. 74-80.
Kandiah PA, Nanchal R, Subramanian RM. Acute Liver Failure. In: Schmidt GA, Kress JP, Douglas IS. eds. Hall, Schmidt and Wood’s Principles of Critical Care, 5th Edition. McGraw Hill; 2023. Accessed August 09, 2023.
CRRT in ALF
Warrillow S, Fisher C, Tibballs H, et al. Continuous renal replacement therapy and its impact on hyperammonaemia in acute liver failure. Crit Care Resusc 2020;22:158-165.
Cardoso FS, Gottfried M, Tujios S, Olson JC, Karvellas CJ, Group USALFS. Continuous renal replacement therapy is associated with reduced serum ammonia levels and mortality in acute liver failure. Hepatology 2018;67:711-720.
Osmolar Shifts in ALF
Liotta EM, Romanova AL, Lizza BD, Rasmussen-Torvik LJ, Kim M, Francis B, et al.
Osmotic shifts, cerebral edema, and neurologic deterioration in severe hepatic encephalopathy. Crit Care Med. (2018) 46(2):280–9. doi: 10.1097/CCM.0000000000002831
Ammonia toxicity in Liver Failure
Dasarathy S, Mookerjee RP, Rackayova V, Rangroo Thrane V, Vairappan B, Ott P, et al. Ammonia toxicity: from head to toe? Metab Brain Dis. (2017) 32(2):529–38. doi: 10.1007/s11011-016-9938-3
Guo, R.M., et al., Brain MRI findings in acute hepatic encephalopathy in liver transplant recipients. Acta Neurol Belg, 2018. 118(2): p. 251-258
Kumar G, Taneja A, Kandiah PA. Brain and the Liver: Cerebral Edema, Hepatic Encephalopathy and Beyond. Hepatic Critical Care. 2017 Aug 7:83–103. doi: 10.1007/978-3-319-66432-3_8. PMCID: PMC7122599.
Ammonia in Cirrhosis
Gallego JJ, Ammonia and beyond – biomarkers of hepatic encephalopathy. Metab Brain Dis. 2025 Jan 15;40(1):100. doi: 10.1007/s11011-024-01512-7. PMID: 39812958; PMCID: PMC11735499.
Ammonia in in post bariatric surgery hyperammonemia
Kamel AY, Shah P, Pipek LZ, Shah A, Kandiah PA. Nutritional Emergencies. Current Surgery Reports. 2025;13(1):30. DOI10.1007/s40137-025-00465-9
Post Lung Transplant Hyperammonemia
Kamel, A.Y., et al., Hyperammonemia After Lung Transplantation: Systematic Review and a Mini Case Series. Transpl Int, 2022. 35: p. 10433.
Post cardiac arrest Hyperammonemia
Nojima T et al. Can Blood Ammonia Level, Prehospital Time, and Return of Spontaneous Circulation Predict Neurological Outcomes of Out-of-Hospital Cardiac Arrest Patients? A Nationwide, Retrospective Cohort Study. J Clin Med. 2022 May 4;11(9):2566. doi: 10.3390/jcm11092566. PMID: 35566692; PMCID: PMC9105173.
Ammonia Bowel Ischemia
Watari M et al. Ammonia determination as an early indicator in experimental superior mesenteric artery occlusion. Hiroshima J Med Sci. 1997 Dec;46(4):159-67. PMID: 9538566.
Study on undifferentiated causes of hyperammonemia
Maquet J et al. Clinical, biochemical, and molecular findings in adults with hyperammonemia: A French bi-centric retrospective study. Mol Genet Metab. 2025 Sep-Oct;146(1-2):109223. doi: 10.1016/j.ymgme.2025.109223. Epub 2025 Aug 13. PMID: 40834544.
Sakusic A, Features of Adult Hyperammonemia Not Due to Liver Failure in the ICU. Crit Care Med. 2018 Sep;46(9):e897-e903. doi: 10.1097/CCM.0000000000003278. PMID: 29985210; PMCID: PMC6095817.
Takeaway lessons
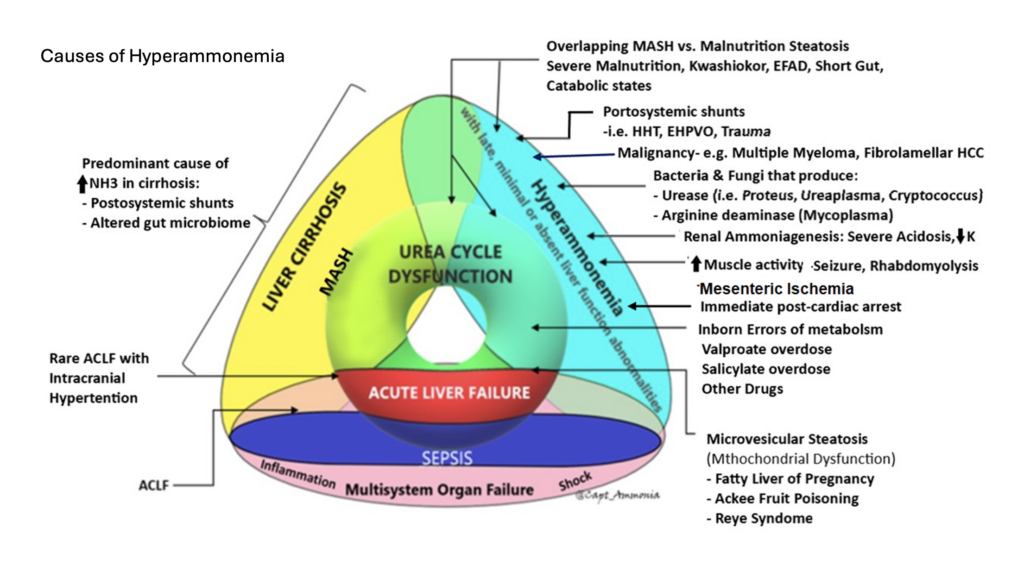
Effective ammonia clearance requires liver function, kidney function, gut function, and presence of skeletal muscles. It can also be compromised by A-V shunting bypassing the portal venous system (i.e. from enteric to systemic circulation; ask your radiologist to look for this as they may not otherwise report it).
Measuring the plasma ammonia level is not too technically difficult, but does have a time limit; allowing a sample to sit may falsely elevate the result. It’s therefore tough to do for outpatients. For inpatients, however, unless it gets forgotten on a table, it is generally not so difficult. Arterial vs venous doesn’t matter.
The peak ammonia on admission for cirrhotics is not as relevant as their cumulative ammonia burden over time (though of course this is not measurable). While difficult to interpret for those patients, a very high number is still very toxic, a very normal level probably absolves hepatic encephalopathy as a cause of altered mental status, and trending a number in between may help confirm response to therapy (eg the number should come down). A persistently elevated ammonia despite adequate catharsis may indicate need for a more aggressive regimen, or other attention to the underlying cause; a common cause would be a patient with GI bleeding, where persistent blood in the gut can cause persistent ammonia elevation.
Everyone agrees that ammonia should be followed in acute liver failure, where it correlates closely with risk of cerebral edema.
Checking ammonia in the patient without clear liver failure, but unexplained altered mental status, is reasonable—though an abnormal result will require a thoughtful approach to explaining it.
Cardiac arrest, especially with prolonged resuscitation, will reliably increase the ammonia level (if measured during or immediately after), as a direct effect of global ischemia.
Gut ischemia can elevate ammonia. Enterocytes require glutamine for energy; by interrupting this pathway, they may generate ammonia via anaerobic metabolism, much as other cells might generate lactate.
Medications, particularly valproate, can elevate ammonia.
Any elevated muscle activity or muscle breakdown, such as seizure or rhabdomyolysis, can generate nitrogen and hence transient hyperammonemia.
Any sarcopenia predisposes to hyperammonemia, as skeletal muscle is too sparse to reliably clear ammonia.
Inborn errors of metabolism involving the urease cycle are uncommon in adults but something to consider, especially if genetic testing is available to you.
Severe malnutrition, most often due to gastric bypass, can cause hyperammonemia. This is probably due to multifactorial causes, including sarcopenia and muscle catabolism, but malnutrition seems to induce a true hepatic steatosis is well (reversible if nutrition is restored). Radiographically and clinically this looks like MAFLD/MASH, but is not caused by metabolic syndrome or obesity, but the opposite state of malnutrition. (This phenomenon is also seen in Kwashiorkor.) Probably this is due to some synthetic dysfunction affecting beta oxidation and lipid metabolism, and/or absence of essential fatty acids—not clear.
Urease-producing bacteria can generate ammonia. This will usually be transient, since antibiotics will readily kill them. However, with a deep-seated infection such as an abscess, this may not be true and should be considered as an ongoing ammonia source. Examples include: Staph epidermidis and Staph saprophyticus, Helicobacter Pylori, Klebsiella, Nocardia, Cryptococcus, Pseudomonas spp., Corynebacterium, Proteus penneri, Providencia stuartii, and Morganella morganii
An especially important urease producer is ureaplasma, an atypical organism similar to mycoplasma, usually causing UTI or even STI. This will often not cause other signs of clinical infection, but can be a cause of ammonia production, and will not be grown on routine cultures (PCRs are needed on urine or BAL, or the Mayo Clinic has a blood PCR—all send-outs), nor covered with routine antimicrobials (atypical coverage, such as doxycycline, azithromycin, or levofloxacin is needed). This infection mostly occurs in the immunosuppressed, such as transplant patients, where it can cause occult pneumonia (an important and morbid cause of post-transplant hyperammonemia); consider it as well in anybody on rituximab or similar immunosuppression. It can also cause “sterile” joint effusions, so a patient on rituximab whose joint is tapped and grows inflammatory-but-aseptic fluid may be presumed to have progression of an underlying rheumatologic disease, have their immunosuppression escalated, and then end up with disseminated ureaplasma.
For the hyperammonemic due to malnutrition/gastric bypass: nourish with glucose and fats while limiting or holding protein completely in the acute period. This can be parenteral initially, as it’s easy to titrate protein in that fashion. Check and/or supplement everyone with micronutrients likely to be insufficient: high-dose thiamine, B6, L-carnitine, copper, zinc. Once ammonia stabilizes and clears, start to introduce protein cautiously, with the goal of eventually restoring an anabolic state to reverse the underlying steatosis. Go slow weaning everything to avoid rebounds.
Refractory hyperammonemia can be treated with dialysis (CRRT), though data is limited in this setting. Starting earlier may make sense, as osmolar clearance may be rapid once initiated and could precipitate cerebral edema if the osm load is already high. Some would add hypertonic saline with CRRT to try and mitigate this rapid osm drop, a common tactic in the ALF realm.
A common cause of proximal decompensation for these people is when micronutrient deficiencies starts to reduce gut motility, leading to poor tolerance of oral nutrition and anorexia. Once you fix these and the gut allows oral intake, their nutritional status can improve.
Lactulose and rifaximin can have some temporizing role in these patients, but a very short-acting one. They may also tend to worsen nutrition by accelerating gut transit time and filling the small-volume stomach.
The urease cycle scavengers sodium phenylacetate-sodium benzoate may help accelerate clearance of ammonia, if renal function is intact (they convert ammonia to PAGN which can be renally cleared). However, they are not a magic solution, take time to work, and do not address the underlying problem.
We dive into the common dilemma of when to give stress-dose corticosteroids in septic shock, with Dr. David Janz, pulm/crit intensivist with a Masters of Science in Clinical Investigation, former director of the Clinical Research Unit for the critical care section at LSU, founding member of the Pragmatic Critical Care Research Group, and associate Chief Medical Officer for LCMC.
The purported effect of corticosteroids in septic shock is to increase sensitivity of peripheral catecholamine receptors, either to endogenous or exogenous adrenergic hormones.
In the four large RCTs of this topic, two showed a beneficial outcome effect and two did not. The two positive trials also added fludrocortisone to the backbone steroid (usually hydrocortisone), though it seems dubious that this was the key difference (fludro has also been studied separately without effect). Those trials also generally enrolled sicker patients, i.e. on higher doses of pressor and more organ failure.
It is probably reasonable to add steroids when on escalating doses of your first-line pressor (e.g. norepinephrine), or when thinking of adding vasopressin, though the SCCM/Surviving Sepsis guidelines now suggest just giving steroids to everyone in septic shock, presumably to simplify decision-making, particularly for non-experts.
Most trials have used hydrocortisone 50 mg q6h or thereabouts, or an equivalent dose as a continuous infusion. The latter makes some physiologic sense but has not been shown to be beneficial head-to-head trials. Most likely, the exact dosing strategy is not too important. Alternate steroids are probably also reasonable, i.e. any moderate-dose parenteral corticosteroid probably gets you the desired effect.
Many trials continued steroids until the patient left the ICU, even if pressors have been weaned off. Most clinicians would probably stop them sooner than this, although we should acknowledge that their effect in raising blood pressure is reliable (sometimes helping to discontinue pressors as much as several days sooner), so continuing them longer could conceivably help with disposition (i.e. help them leave and stay out of the ICU), which is a good thing for hospitals and probably patients.
Dr. Janz stops steroids when the pressors are stopped, with no taper or wean. Some would do a short taper, but the more complex you make the process in a busy ICU, the more likely that someone will forget to discontinue them altogether, and that the patient will stay on steroids for their whole hospitalization (or forever). There is no physiologic suppression of the native steroid production with these durations of steroid therapy (usually 3-4 days, almost always <1 week), and an abrupt halt is what was done in the trials.
Etomidate has been repeatedly shown to cause a measurable decrease in cortisol levels, even after single doses (e.g. for intubation). However, this has not been shown to be associated with any negative outcome (most recently in the EVK trial).
There is very little data on whether steroids should be used in shock from other etiologies. It may make some sense in other inflammatory states, such as pancreatitis, post-CPB vasoplegia, etc. But we really don’t know. In a mixed shock state where sepsis is present along with something else like cardiogenic shock, Dr. Janz uses steroids; otherwise no.
Whether to always augment the home steroid dose in chronic steroid users, even without shock, has shifted—in the past, endocrinology guidelines were to always do this empirically (e.g. in steroid users undergoing surgery or some other stressor), now they still generally favor this but are moving towards increasing the home dose only if signs of adrenal crisis develop.
We explore the fascinating intricacies and unique features of the burned critically ill patient, with Clint Leonard, NP in the burn ICU at Vanderbilt and ABLS instructor.