We explore the cutting edge practice of point-of-care ultrasound of the brain, including optic nerve sheath measurement, transcranial doppler, assessing midline shift, and more, with Aarti Sarwal, neurologist and neurointensivist, director of the neurocritical care unit at Wake Forest, and director of their neurovascular lab and ultrasound courses.
POCUS can potentially be used to identify elevated ICP by optic nerve sheath ultrasound or pupillary assessment (in patients with difficult-to-assess pupils due to edema or other factors). Midline shift can be seen and quantified via the temporal window, and hemorrhagic masses can potentially be visualized. Finally, spectral doppler of the cranial vessels can show changes in intracranial compliance, similar to that seen in formal TCDs during vasospasm.
Learning curve for these studies is probably around 50-100 studies until competence, but may be creeping closer to 30–50 and eventually lower due to improving education, and increasing awareness and skills with the general concepts being applied.
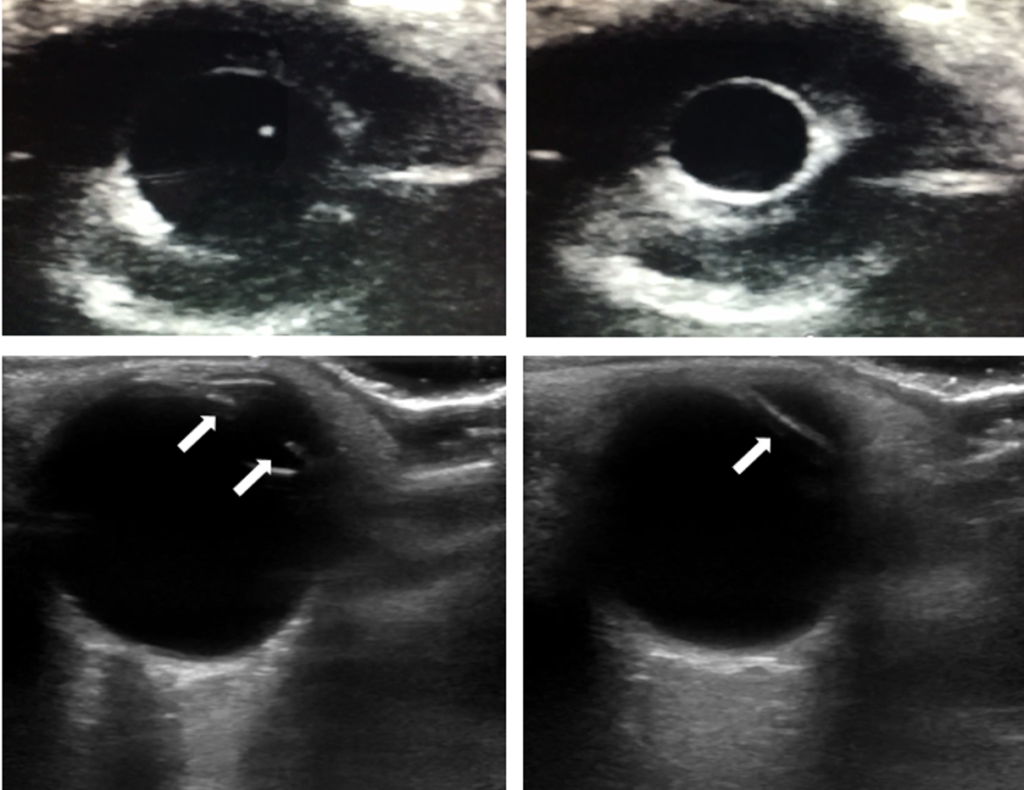
The linear probe can be used over a closed eyelid to visualize the iris, allowing assessment of pupil response when light in shined in the opposite eye; this can be useful when the lid cannot be opened, such as from edema or trauma. M-mode can even be used for quantitative pupillometry.
An increased diameter of the optic nerve sheath measured 3 mm from the globe (using the linear probe in a transverse, ear-to-ear axis) correlates with increased intracranial pressure, as the sheath is a continuation of the cranial space and tends to swell with higher ICP. Papilledema can also be seen here as bulging of the optic disc. Use the orbital or ocular preset, which reduces power (mechanical and thermal indexes) delivered to the eye.
A cutoff reflecting elevated ICP is usually somewhere in the 5-7 mm range. However, normal values vary a lot, and very acute ICP crisis can choke off the continuity and cause normal diameters, so simple measurement can imperfect (analogy: IVC measurement). Trending can be more useful if you can establish a baseline, and papilledema is somewhat more specific. In pediatrics, adjusting for head circumference can help.
Slower increases in ICP tend to be associated with larger optic nerve sheath diameters, whereas rapid increases may actually be associated with normal sheath diameter, due to edema at the basal cistern level choking off communication with the cranial vault.
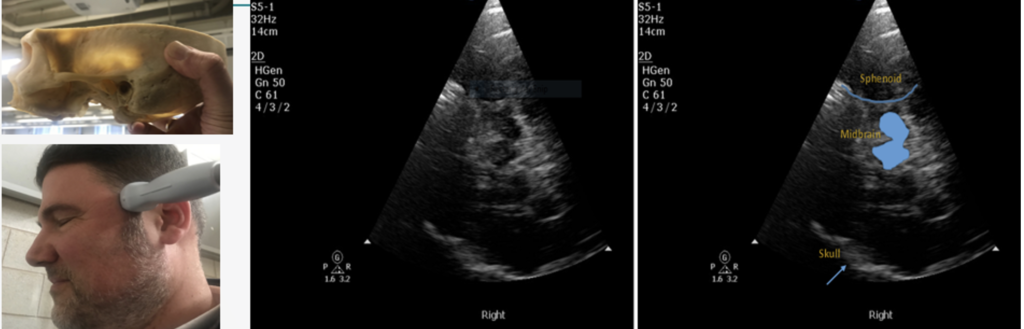
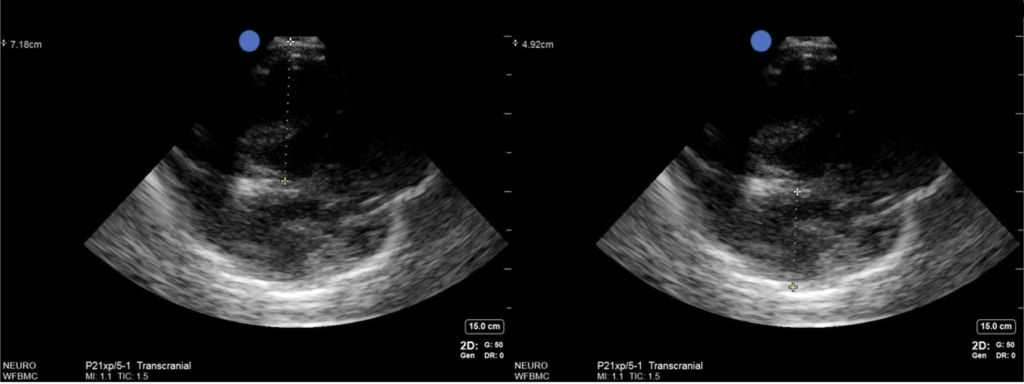
Midline structures like the pineal gland, third ventricle, or septum pellucidum can be seen from the temporal ultrasound window; 85-95% of the population will have adequate windows here, at least on one side, with some decrease in old age. Males tend to have worse windows, windows worsen over time, and there is some ethnic variation.
Research is early, but distance of the midline structures from the probe can be compared with their distance from the opposite skull (i.e. in the deep field). Differences between the two can help diagnose and quantify midline shift. Caveats: it’s difficult to establish exactly the same angle when insonating opposing sides, and identical angles can be impossible due to limitations in the windows, so don’t compare that way. The region of edema may mean different structures are shifted while others are normal, or even that there is no shift (e.g. herniation is not lateral); ideally, pick a midline structure that makes sense for where their pathology is found. This is probably more useful for serial comparisons than absolute values, since your angle that penetrates the small temporal window will usually not be perfectly flat, but will be reproducible.
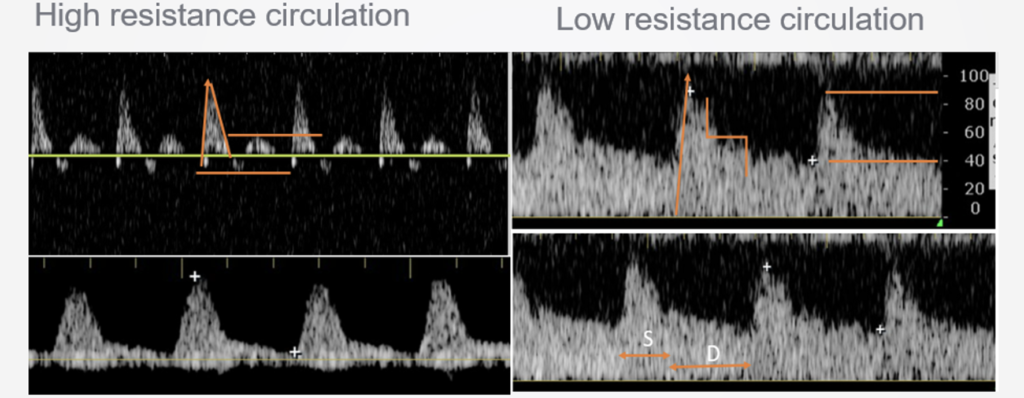
Global edema may not be seen in midline shift, but may be seen in the TCD waveforms. Spectral doppler of vessels like the MCAs should show low resistance waveforms in a normal brain (low systolic peaks, a long runoff and high diastolic), while in a tighter brain with higher ICP, resistance gets worse, with a higher systolic, quicker drop, and lower diastolic pressure, all the way up until diastolic pressures become less than zero and flow is oscillating (e.g. back-and-forth during the cardiac cycle, which reflects no overall flow and is consistent with brain death). TCD measurements can be directly extrapolated to ICP using a number of published formulas.
Research is early, but transtemporal B-mode seems to have good sensitivity (>95%) for detecting parenchymal hemorrhage in the brain, as long as it is large and fresh; new blood shows up as a hyperechoic lesion with shadowing.
We chat with friend of the podcast Matt Siuba (@msiuba), Mr. Zentensivist, to share our distinct perspectives on the relationship between APPs (PAs or NPs) and the intensivists we work alongside.
We dive into when to initiate renal replacement therapy, the modalities, settings, and physics involved, troubleshooting problems, and more, with Dr. Paul Adams, a dual-trained nephrologist and intensivist at the University of Kentucky.
One of the better indications for early dialysis in the ICU patient is to control volume, which in an oliguric patient you know is likely to keep accumulating.
Help determine who is likely to eventually need dialysis (and hence deciding early vs late, not early vs maybe never) with a furosemide stress test: give 1-1.5 mg/kg of furosemide (160 mg is often about right), then if they don’t make about 1 ml/kg/hr of urine for a few hours, they’re likely to end up needing renal replacement therapy.
Realistically, most true indications for acute dialysis in the ICU are hyperkalemia, volume overload, or occasional toxicology.
CRRT is generally more effective at volume management, particularly preemptive volume management, because it continues throughout the day and can more easily keep up with inputs. It is also more hemodynamically stable.
CRRT can be done via CVVH (using convective flow to drag out fluid and solutes via pressure across a filter), CVVHD (using diffusion gradients to clear solute and fluid), or CVVHDF (using both). Which modality of CRRT is used tends to come down to institution and practitioner practice, although there are some clinical differences in amount of solute clearance and such.
Effluent is the balanced electrolyte fluid which is used for therapy, and can be run into the blood before reaching the filter (diluting it and improving filter life, but decreasing efficiency), after reaching the filter (purely to replace what was lost), and on the other side of the filter (creating a dialysis effect). Total effluent rate gets divided among these sites as you like.
UF (ultrafiltration) is essentially whatever fluid is lost that you’re not replacing.
About 25–30 ml/kg/hr is usually about the right effluent rate. A higher rate helps make up for interruptions during the day.
150–250 ml/hr bloodflow is about right; it generally has relatively little effect on clearance in CRRT (unlike in intermittent HD, where it directly impacts clearance).
Circuit life can be prolonged with anticoagulation. Heparin can be used either systemically or regionally (infused at the start of the circuit, then reversed at the end using protamine), or citrate can be used regionally (replaced with calcium at the end), although it requires close monitoring of ionized calcium levels (really the ratio between total and ionized calcium, since citrate-bound calcium still registers on total calcium assays; a total calcium more than 2-2.5x higher than ionized levels suggests citrate toxicity).
16–18 hours of CRRT is usually needed before you start to see an impact on serum solute levels. For critical levels like severe hyperkalemia, start with IHD instead to get a quick correction.
Pressure problems at the dialysis access are almost always due to anatomic issues like catheter placement. Try adjusting the line, such as placing it deeper. Reducing bloodflow may help, using a different site, or rarely pharmacologically paralyzing the patient.
Pressure problems at the filter (“transmembrane pressure” or TMP) are usually from clotting. Consider anticoagulation if not already being used, or pre-filter fluid. Inflammatory patients like in sepsis can have very dirty, clotty blood.
If a patient starts making 600-1000ml of urine daily, consider weaning of renal replacement. That is not common in the critically ill, even if they eventually have later renal recovery; transition to IHD is more common.
If volume inputs are still ample (many liters a day), it’ll be hard to keep up using IHD, since UF rates top out around a liter per hour. Stick with CRRT in that case.
Rhabdomyolysis “disproportionately” increases BUN and creatinine, since those are products of muscle breakdown; they may have adequate renal function (demonstrated by robust urine output) despite high numbers.
We chat with Callie Tennyson, DNP, ACNP-BC, AACC, CHSE, assistant professor from the Duke University School of Nursing, about the use of the internet and social media for medical education: trends, challenges, and principles for doing it right.

{kind=link}