Brandon walks Bryan through a case of new, unexplained hypotension in the ICU, with a focus on approaching shock, the use of POCUS, and risk stratifying unexplained problems.
Takeaway lessons
Sudden changes in vital signs or other status are often due to precipitating factors, such as iatrogenic stimuli, whereas more gradual changes are often due to evolution of the underlying diseases. This is not always reliable.
Sudden changes can also be due to monitoring artifacts, such as inaccurate telemetry, problematic arterial lines, etc.
Failing arterial lines are usually damped (reduced amplitude), causing depressed systolic pressures and raised diastolics, but the MAP still tends to still be reliable.
Hypotension with a narrower pulse pressure is somewhat more suggestive of hypovolemia than vasodilation. This is not always reliable.
Point-of-care ultrasound is probably the single best tool for assessing unexplained hypotension, mainly because it can (within a few seconds) rule out most of the life-threatening, specifically treatable causes, such as cardiac tamponade, PE, cardiogenic shock, major hemorrhage, and tension pneumothorax. Distributive shock (e.g. from sepsis), while among the most common causes of hypotension in the ICU, is a diagnosis of exclusion.
A fluid bolus used diagnostically should be given fast, and all the faster if you’re not giving very much volume. Use a pressure bag and don’t leave the room.
One of the hardest acts of judgment in a clinician is to recognize whether a new finding is a “big deal” or not.
Discussing ICU triage, risk stratification, and patient disposition with intensivist Eddy Joe Gutierrez (@eddyjoemd) of the Saving Lives Podcast.
For 20% off the upcoming Resuscitative TEE courses (through July 23, 2022), listen to the show for a promo code for CCS listeners!
Takeaway lessons
When a patient has borderline indications for requiring the ICU, generally, in the real world, they should go to the ICU. More often than not, “downtriage” results in a later, inevitable, yet delayed upgrade to the ICU.
Sometimes, borderline patients may need the ICU just to complete the workup and prove that they don’t need the ICU. This is annoying but inevitable; such patients can’t languish for a 12-hour evaluation in the ED no matter how much we might want them to. The ED needs to flow, and there’s no better diagnostic tool than time.
A good practical rule for which pulmonary emboli require the ICU are those that will, or may, require an intervention other than systemic anticoagulation. Examples include systemic thrombolysis, catheter-directed thrombolytics, thrombectomy, etc.
In theory, patients with a downward trajectory can remain outside the ICU until they reach the point where they require critical care, then can be upgraded. This can work as long as their deterioration is controlled and not precipitous, i.e. there’s time to safely recognize their status and move them to higher care when the time comes. But this is often not easy to know.
The location of care can influence care in non-obvious ways. For instance, a septic patient may receive excessive harmful IV fluid boluses as providers attempt to avoid an upgrade to the ICU to administer vasopressors.
Bed availability has no relation to patient disposition, other than the fact that patients forced to board outside the unit will probably, inevitably receive worse care.
The readiness to transfer a patient from the ICU is usually higher than the threshold for accepting them initially. This isn’t a fallacy. It’s due to the fact that the former has had a period of observation, whereas the latter has not yet demonstrated their trajectory.
When a sending provider (e.g. in the ED, floor, or an outside hospital) thinks a patient needs the ICU, and you don’t think so, they usually should win. A patient may not need the ICU, but if they can’t stay where they are, uptriage is the safety net.
Ultimately, safe triage is usually a process, not a snapshot, and patients may need to move more than once. Smooth and safe transfers of care usually comes down to details and knowledge of your specific institution, and navigating it well requires good communication. Teams that can’t talk to each other inevitably lead to deficiencies in care.
Making certain triage determinations by policy, committee, or guideline can help counteract the natural tendency (at least in the US) to always overtriage due to concern about personal provider risk.
Try to limit your second-guessing about other people’s triage decisions made in retrospect. It’s a lot easier after the fact.
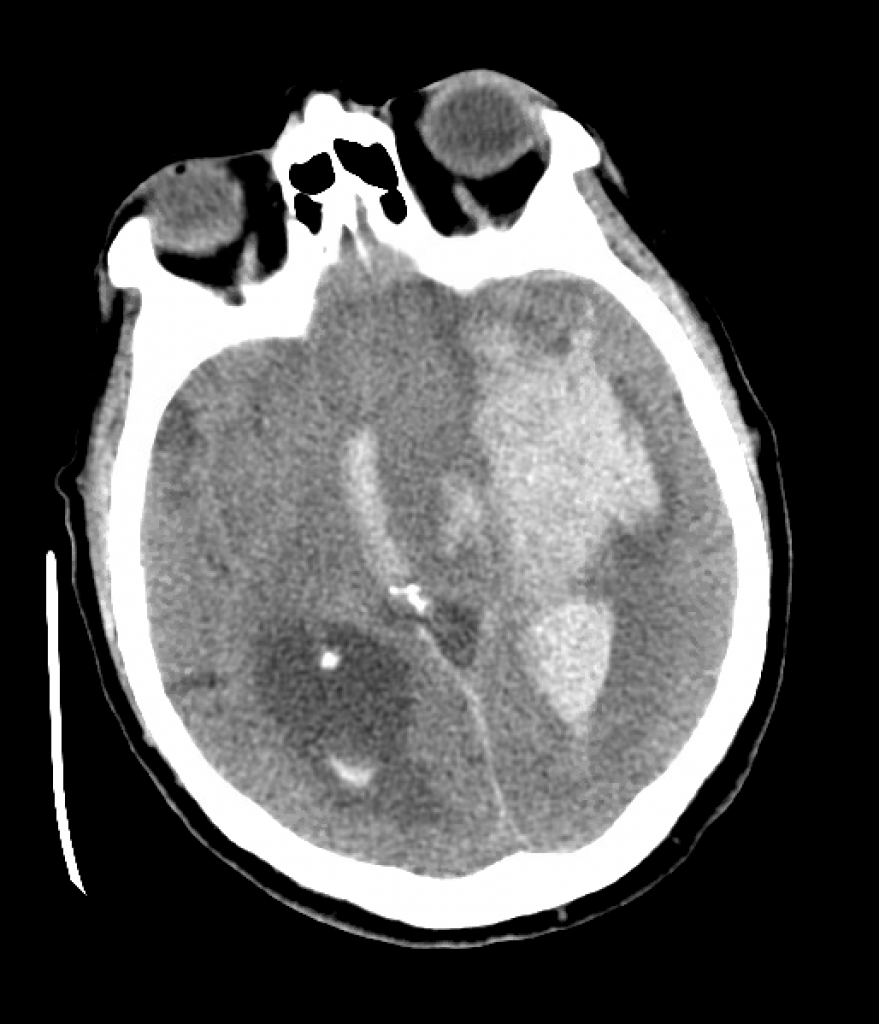
We review a case of massive intraparenchymal hemorrhage progressing to brain death, including the process of brain death testing and declaration, with Dr. Casey Albin (@CaseyAlbin), neurologist and neurointensivist, assistant professor of Neurology and Neurosurgery at Emory and part of the NeuroEmcrit team.
For 20% off the upcoming Resuscitative TEE courses (through July 23, 2022), listen to the show for a promo code for CCS listeners!
Takeaway lessons
In general, in patients with good baseline function, it’s reasonable to be fairly aggressive with initial care, such as placement of intracranial pressure monitors, even if long-term goals of care are unclear—it can always be escalated.
Although ICH score is associated with mortality, the original study allowed withdrawal of care at discretion of the clinicians, so the data may be tainted by self-fulfilling prophecy—withdrawal of care may lead to poor prognosis in some cases, not always the reverse.
Sodium goals are ideally titrated to ICP (with invasive monitoring). In its absence it’s best to target clinical findings, unless you have tools like TCDs or optic nerve sheath ultrasound, or just frequent CT scans. Arbitrary sodium goals are rarely helpful.
There is good evidence for decompressive hemicraniectomy for large MCA infarct IF the patient is young; it is less clear in the elderly. If it’s going to be done, do it early.
If herniation is clear via ICP or imaging, don’t spare sedation for the sake of a neuro exam, unless you’re at the point of stepping back and assessing for long-term futility and possible brain death.
4-5 days into admission is often when families begin to understand the nature of a devastating neurologic injury. In some cases, discussion of futility and brain death may be initiated by families after doing their own research.
The first step is holding sedation and waiting ~5 half-lives for confounding drugs to clear; impaired renal or hepatic clearance should be taken into account here. (Pharmacy may be helpful.) Paralysis should be held and train-of-four can be used to confirm. Drug levels can be used to confirm clearance of opioids, etc if needed.
The law (Uniform Declaration of Death Act) doesn’t always agree with guidelines (while hospital policies may differ even further). The UDDA requires complete brain death, whereas the AAN’s guidelines don’t necessarily require pituitary death (patient need not be in DI), but all do require more than just brainstem death—for example, a locked-in patient would not qualify.
Expect and manage DI, as hypovolemia and hypernatremia may make the patient too unstable to tolerate brain death testing. Consider a vasopressin drip, replace volume, etc.
As the chest wall becomes denervated, it loses elastic recoil, while hypovolemia may cause very hyperdynamic cardiac function. The combination can cause strong chest wall vibrations which may autotrigger the ventilator, often confusing staff and family who believe the patient is breathing spontaneously.
Perform brain death testing in a systematic, scrupulous manner. Print your hospital policy and use it as a formal checklist. You’ll need a bright penlight, a tongue depressor or Yankhauer catheter, a Q-tip or gaue for corneal reflexes, 50 ml x2 of ice-cold water and a syringe with an IV catheter on the tip for cold calorics, and some kind of insufflation catheter or a T-piece for apnea testing.
Pitfalls: remember to test corneals by touching the actual cornea, not the sclera. Cold calorics are performed by irrigating the ear canal and watching for gaze deviation (any deviation shows brainstem activity). Gag reflex must be checked all the way in the back of the oropharynx with vigorous stimulation. Cough and pain responses must also be checked with substantial stimulation. Warn family ahead of time about the possibility of purely reflexive triple flexion.
Consider bringing the family to watch, which helps encourage transparency. Warn them ahead of time that if the test is confirmatory, it will indicate the patient is dead by brain criteria.
You generally want an arterial line for the apnea test, and have vasopressors running and ready to maintain the SBP >100. Put the patient on 100% FiO2 and get a baseline ABG showing normocapnia and a PAO2 >200. (If the patient has a baseline elevated PACO2, follow your local policy.) Oxygenate the patient passively, such as by inserting an insufflation catheter hooked up to oxygen down the ET tube after disconnecting the ventilator. Uncover the patient’s chest and watch for chest rise.
A confirmatory apnea test is one where the PACO2 rises by 20 points, without any clinical signs of breathing; hence the team needs to be in the room, physically observing the patient. An equivocal test is one where the test cannot be completed or the PCO2 fails to adequately rise to confirm adequate levels. Most tests are completed by 10 minutes, but start sending blood gasses earlier than that (e.g. at 6, 8, 10 minutes), as you may need to terminate the test due to instability while waiting for the most recent gas and you’ll want to know if the patient had finished.
Confirmatory/ancillary tests can be done if the clinical and apnea tests cannot be done, or are not completely definitive due to confounding factors. They can include TCDs, nuclear flow studies, or EEG if specialized equipment and readers are available. Catheter-directed 4-vessel cerebral angiography is another option, but CTA/MRA are not. Most of these tests are looking for intracranial circulatory arrest, i.e. lack of blood flow to the brain—dead cells have no metabolic demand and shunt blood away.
Perform brain death testing as soon as clinically appropriate; they only become more unstable.
Resources
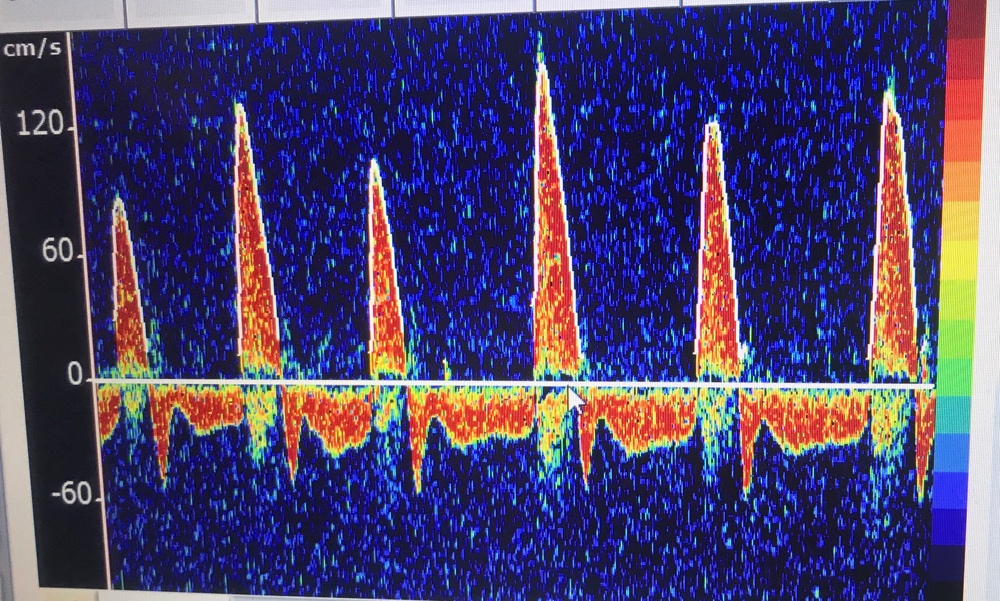
An example of massive ICH with IVH.TCDs in brain death, with sharp systolic spikes and diastolic flow reversal
We discuss the clinical presentation and management of AFE with guests Dr. Stephanie Martin (Twitter: @OBCriticalCare, Instagram: @criticalcareob), medical director for Clinical Concepts in Obstetrics and a Maternal Fetal Medicine specialist in Scottsdale, Arizona with expertise in critical care obstetrics. She is also co-host of the Critical Care Obstetrics podcast. We’re also joined for a patient perspective by Miranda Klassen (@afefoundation), Executive Director of the AFE Foundation, and her husband Bryce Klassen, CCRN, ICU Supervisor at Scripps Memorial Hospital Encinitas.
Takeaway lessons
AFE is poorly understood but is probably caused by exposure of amniotic fluid (skin cells, hair, vernix, etc) to maternal blood, causing a severe inflammatory reaction. Although it may contribute, it is probably not mainly due to obstructive shock, as seen in pulmonary embolism.
AFE is rare. Some clinicians will go an entire career without seeing it. However, it certainly happens and has tremendous consequences when it does.
As a rule, ACLS care is the same for pregnant women. The main exception is that if ROSC is not obtained immediately, you must perform a resuscitative Caesarean section within the first 4 minutes, aiming to have the baby delivered within 5. Without this, the chances of recovering the mother are slim: the gravid uterus interferes with compressions, compresses the IVC, and causes other problems. Achieving this in non-obstetric areas requires a carefully thought-out process. Time must not be wasted transporting the patient elsewhere. The only equipment absolutely required is a scalpel, although this too can be hard to find if you haven’t optimized your process. In short, if you have a pregnant woman in your ICU, figure out now what you’re going to do now if she codes.
Due to the logistical challenges, most of these resuscitative C-sections are actually done in 6-15 minutes. This is not the goal.
During CPR, the gravid uterus should be manually displaced to one side, preferably the left. (It is no longer recommended to tilt the patient laterally, since this interferes with compressions.)
AFE is rare, but with excellent care it is survivable.
Bleeding post C-section is usually not significant. The abdomen can be left open, and can even be used for aortic access to check for the pulse, or occlude the aorta (either manually or by cross-clamp).
A normal fibrinogen level in a pregnant or immediately post-partum female is elevated (often in the ~600s), so a “normal” level should be considered low. Use this to follow DIC. Bleeding and clotting may both occur.
Although pregnant women have a subtle physiologic hemodilution, their normal hemoglobin should not drop below 11, so for our purposes, anemia still denotes anemia.
Resuscitating the immediately post-partum woman should not mean great confusion about safe medications. Use whatever is necessary to save her life. Any impacts on breastmilk can be managed by pumping and either saving or dumping it as appropriate.
A compensated respiratory alkalosis via hyperventilation should be expected during pregnancy (the mother must have a lower PCO2 than the fetus to create a gradient for fetal ventilation). This persists post-partum, so it’s probably appropriate to aim to maintain this by increasing minute ventilation, even although it’s likely not as critical since there’s no longer a fetus to support.
The most important post-partum care after an emergency like this remains supportive critical care. Eventually the mother can be transferred to a post-partum obstetric unit, but these are not high acuity floors (with nurse:patient ratios as high as 8:1) and this needs not be rushed. OB staff can come to the ICU to assist and educate as needed.
If you have a suspected AFE, call the AFE Foundation 24/7 (307-363-2337) for advice and to coordinate collection of specimens, which must be done promptly and is badly needed to improve our understanding of this disease.
References
Amniotic fluid embolism: principles of early clinical management. Pacheco, Luis D, Klassen, M., et. al. American Journal of Obstetrics & Gynecology.
Society for Maternal-Fetal Medicine (SMFM). Pacheco LD, Saade G, et al. Amniotic fluid embolism: diagnosis and management. Am J Obstet Gynecol 2016; 215:B16.
Stafford, IA, Moaddab, A, Dildy, GA (2019) Evaluation of proposed criteria for research reporting of amniotic fluid embolism. AJOG, 220, 285-287.
Combs CA, Montgomery DM, Toner LE, Dildy GA, Patient Safety and Quality Committee, Society for Maternal-Fetal Medicine, Society for Maternal-Fetal Medicine Special Statement: Checklist for initial management of amniotic fluid embolism, American Journal of Obstetrics
Amniotic fluid embolism: Pathophysiology from the perspective of pathology. Tamura N, Farhana M, Oda T, Itoh H, Kanayama N. J Obstet Gynaecol Res. 2017;43(4):627. Epub 2017 Feb 11.
Kiranpreet, K., Bhardwaj, M, Kumar, P., Singhai, S., Singh, T., & Hooda, S. (2016). Amniotic fluid embolism. J Anesthesiol Clin Pharmacol, 32(2), 153-159.
Zelop CM, Einav S, Mhyre JM, Lipman SS, Arafeh J, Shaw RE, Edelson DP, Jeejeebhoy FM; American Heart Association’s Get With the Guidelines-Resuscitation Investigators. Characteristics and outcomes of maternal cardiac arrest: A descriptive analysis of Get with the guidelines data. Resuscitation. 2018 Nov;132:17-20. doi: 10.1016/j.resuscitation.2018.08.029. Epub 2018 Aug 28. PMID: 30170022.
A look at rehabilitation and mobility in the critically ill, from the perspective of our skilled therapists—with Heidi Engel, PT, DPT of UC San Francisco, long-term provider of acute care therapy, researcher in ICU rehabilitation, and founding member of the SCCM’s ICU Liberation program.
Takeaway lessons
Tolerance of pressure support ventilation is often a good marker that a patient is ready to start meaningful PT. Before that, the harm may exceed the benefit, unless there’s a specific reason why activity may help move them along, such as attenuating delirium and agitation and improving tolerance of the ET tube.
The most common complaints and stressors of ICU patients are: feeling thirsty, feeling traumatized and afraid, the inability to communicate, and feeling “air hungry” due to the strange mechanics of mechanical ventilation and other respiratory modalities.
In many cases, rehab will require convincing patients to get over an initial hump. Breathing, strength, and discomfort may initially be a challenge but will improve with activity.
You may need to choose priorities: do you want to push vent liberation or mobility today?
Bring the light during daytime hours to improve the circadian rhythm, but direct fluorescent lights are harsh and can encourage closed eyes. Natural, indirect light is better.
Although PT and OT have complementary roles, they will sometimes try to see patients together, which can have downsides by underemphasizing the unique aspects of each role, reducing total rehab time, and relegating one skilled therapist to acting as merely a set of hands.
The presence of any sedation, even “gentle” agents like precedex, creates an obstacle to effective PT.
Getting patients up to a chair helps with agorophobia by changing their perspective from their tiny bed-shaped home.
Heidi’s rehab process
Check the RASS and CAM-ICU scores
Explain to patient the importance of the endotracheal tube and not touching it. Bring all equipment to the side of the bed with the ventilator.
Perform some gastroc/hamstring stretching to initiate mobility and help wake the patient up
Ask them to follow commands, such as: push! Can they follow? Do the vent and vitals remain okay?
Sit them up at edge of bed, arrange equipment. Observe head control, trunk control, breathing, vitals, orthostasis, etc.
bring a big mobility device, see if they can stand.
While they’re up, use the opportunity to clean the linen, wash their face, comb their hair, clean their posterior.
COVID is making it harder, often just for practical reasons: PPE limiting mobility, noise from filters and masks, families not present, weird autonomic and orthostatic issues… all far more time consuming. However, they do get better and many times do very well, sometimes even recovering faster than similar non-COVID patients. Omicron has not been as bad.
Dedicated therapy teams for the ICU add cost, but cost analyses have shown the benefit (in terms of reducing length of stay and other expenses) to actually result in net cost savings.
In-bed, non-weight-bearing activities such as passive range of movement exercise is perhaps better than nothing, but is nowhere near as useful as weightbearing activity out of bed, and has not shown the same clinical benefits in the literature. Every day of out-of-bed activity may pay back several fewer days of rehab down the road.
The hows, whys, logistics, and applications of focused, bedside transesophageal echocardiography performed by critical care and EM providers, with Felipe Teran, assistant professor of emergency medicine at Weill Cornell and director of the Resuscitative TEE Project.
Takeaway lessons
As a rule, resuscitative TEE is performed in patients with a secured airway.
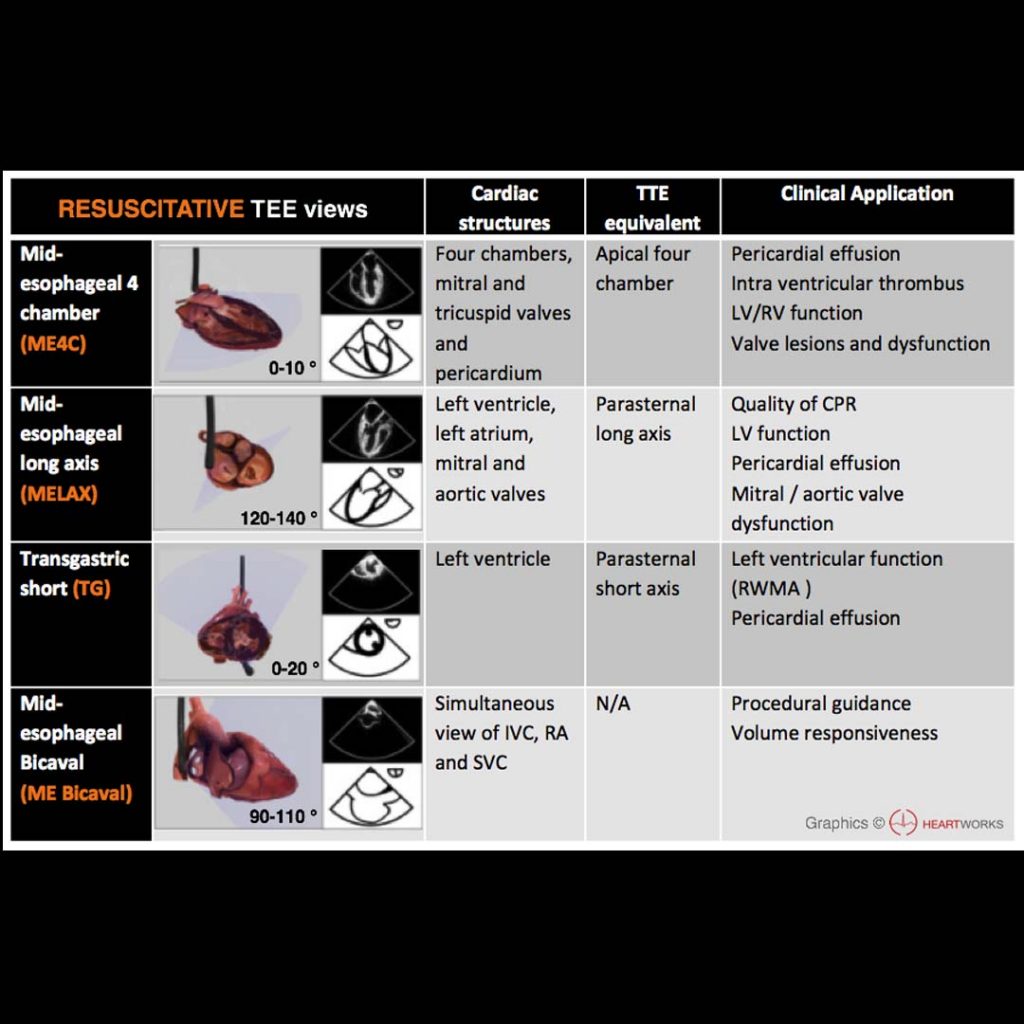
TEE views are not unlike TTE views, just at a different angle (often backwards/upside down down). The technical skills are very similar, and skilled TTE users will find the learning curve short. There are actually fewer probe manipulations (in and out, left and right, and Omniplane rotation, along with some less-used ones like flexion/extension).
The same questions you’d typically ask with TTE can be asked with TEE: is there tamponade? is there cardiogenic shock? is there RV failure? is there hypovolemia? These can be answered even in patients with technically-difficult surface windows.
Some questions hard to answer with TTE can be answered with TEE, such as obtaining reliable RV inflow-outflow views and reliable valve assessments.
Some new questions can be answered with TEE alone: is there aortic dissection? are catheters and wires (ECMO, Impella, pacing wires, etc) optimally placed?
TEE has specific applications in cardiac arrest: are chest compressions optimally positioned on the chest? What is the rhythm? It provides monitoring much more continuous than intermittent TTEs, since it can be left in place.
In an ideal world, resuscitative TEE would be handled very much like TTE, and performed in a similar way—not restricted to some small group of “superusers” or for very rare cases.
When implemented by trained users in appropriately-selected cases (e.g. in shock with inadequate transthoracic windows), it impacts care virtually 100% of the time.
An overview of the role and contributions of a clinical pharmacist in the ICU, with Laura Means Ebbitt of the University of Kentucky, a clinical pharmacist specializing in colorectal/ENT surgery and critical care.
Takeaway lessons
A clinical pharmacist is a “knowledge pharmacist,” dispensing advice rather than medications. They round with the team to review meds and answer questions about routes, interactions, etc, follow up on patient education and post-discharge coordination, assist with medications during cardiac arrests and other emergencies, and provide other clinically-oriented guidance and oversight. Most have completed post-graduate residency programs.
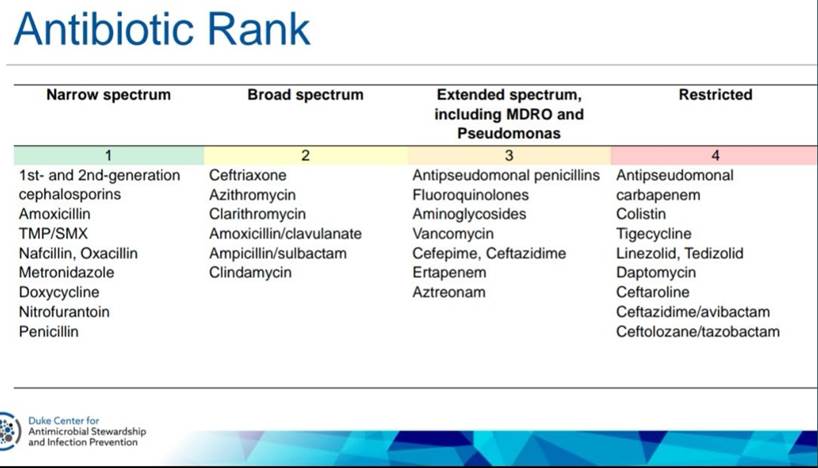
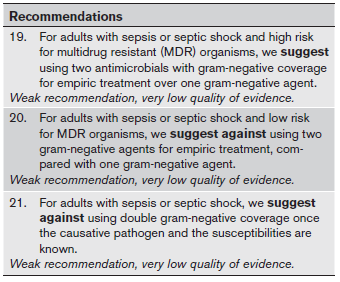
Clinical pharmacists generally have an important role for antibiotic regimen selection, monitoring, and stewardship.
They consider cost in a way that providers rarely do.
They provide patient education that we typically defer or omit.
They’re great at catching deviations in good ICU practices, such as missing DVT or stress ulcer prophylaxis, managing and reconciling home medications, and coordinating nutrition needs (particularly with TPN).
Part two of our discussion with fan favorite Matt Siuba (@msiuba), Cleveland Clinic intensivist, on complications in critical care and how to prevent and manage them. Today we focus on respiratory failure after extubation, and unintentional self-extubation.
Takeaway lessons
When considering extubation of borderline patients, extubating to high flow nasal cannula or CPAP/BiPAP is often a good compromise. This is probably at least a little better than waiting for them to struggle before applying the support, plus it’s easier to assess their course. They can always come off if they look stellar.
Set up for extubation success by first optimizing volume status, sedation strategies, mobility, and other good liberation practices.
If concerned about pulmonary edema, a trial of a “tube compensation” mode alone (versus pressure support with PEEP) may be a good “strict” trial, as compared to more primitive ZEEP or T-piece trials.
Post-extubation stridor is not always predictable, although known airway trauma should raise suspicions. If severe, or even borderline, patients should be promptly reintubated. If more mild, a trial of a couple hours on medical therapies and NIPPV is reasonable. Try steroids (dexamethasone 10 mg IV or so).
Cuff leak tests are not very predictive and as likely to mislead as help. Visual inspection of high-risk airways for laryngeal edema may be helpful, although remember that a large tube in a small airway may never have a leak (and always visually look tight), yet may not be at risk for narrowing after tube removal.
Self-extubation should prompt emergent preparation to oxygenate and reintubate, although you can assess their stability before actually doing it. Remove the tube if still stuck in the mouth. Stop sedative drips that suppress breathing.
If agitation precludes oxygenation, consider antipsychotics. Dexmedetomidine may be useful in this situation, but takes a good 30-60 minutes to get loaded, so you may need another agent as a bridge. Don’t use a loading dose of dex, but starting at a higher rate (>0.6) is smart.
A patient intubated primarily because of agitation will usually do fine after extubation, whether intentional or accidental. The main problem is that agitation precludes a clear, easily-interpretable SBT.
“Extubation hesitancy” is a common error in the ICU. Clinicians are overly hesitant about failed extubations but not worried enough about prolonged intubation courses from the failure to try. Accept that a 0% chance of reintubation means leaving people on the vent for too long; acknowledge risks, plan for fallbacks, and don’t take failure personally; optimize the circumstances; but in the end, try. Risk need not be zero, it should just be lower than the risk of continued mechanical ventilation. “Not everybody is going to be ready every day, but you should treat every day like it’s extubation day.”
The immediacy of the psychological feedback when a patient self extubates gives it primacy and power in our minds. It’s easy to see its harms, while it’s harder to see the harms of the oversedation that prevents it. “Overcautious” is really “overmedicalizing” and is not a safer flavor of risk.
Dr. André Mansoor (@AndreMansoor), associate professor of medicine in Portland, Oregon, author of the excellent Frameworks for Internal Medicine, and contributor to Physical Diagnosis PDX, talks us through a complex case of encephalopathy and respiratory failure to illustrate some principles of diagnostic reasoning.
Takeaway lessons
The hardest part of treating most diseases is making the diagnosis. Countless resources are available to assist with treatment pathways, but you won’t know which one to use if you don’t know what you’re treating. Empiric treatment is sometimes necessary in the critically ill, but it tends to obfuscate, not support diagnosis.
Even diagnostic support tools (such as burgeoning field of artificial intelligence) will require clinicians to collect the contributory data points, such as history and physical exam findings; this still requires enough diagnostic acumen to guide the data-gathering process.
The H&P is not “over” after the initial survey; an iterative back-and-forth process ensues between discovering diagnostic abnormalities and using them to formulate new hypotheses that direct additional, more focused questions and examination.
Most hypoxemia is best approached by first calculating, or at least approximating, the A-a gradient. This routes you into completely different diagnostic pathways depending on the results.
Guillain-Barré is best confirmed by lumbar puncture showing an elevated protein without pleocytosis. However, start with a physical exam suggestive of lower motor neuron disease.
Start with a general history and exam, but after that, broad or “shotgun” testing, consultation, or empiric therapy is high in cost and complications, and just doesn’t tend to work. Formulate specific hypotheses and use your studies or consultations to test them.
90% of diagnoses are made from the history and physical alone. Lean on these as the cornerstone of your diagnostic process, not on high-tech tests.
It’s reasonable to treat a patient who easily matches a standard disease script as if they have the common disease. But when they have features that appear a little different, that’s a good time to step back and work your diagnostic process methodically.
An overview of VV ECMO with a focus on COVID-19, with Dr. Kimberly A. Boswell (EM and CCM) of the University of Maryland, perhaps the busiest center in the country for COVID-related ECMO. We discuss evaluating for candidacy, induction, maintenance, weaning, and general approaches to the COVID patient.
Takeaway lessons
The limited amount of ECMO resources has led to narrowing of criteria. Maryland has reduced their standard upper age limit from <65 to <55, BMI of <40, mechanical ventilation duration <7 days (formerly <10). Also consider other organ failures, as well as duration of symptoms—not just intubation—as a prolonged pre-intubation course suggests a late, potentially fibroproliferative phase of disease which may not be responsive to ECMO.
Almost all COVID cases at Maryland have been VV ECMO; they have very rarely considered VA ECMO. The most obvious indication for the latter would be right heart failure, but in most cases, they would be more likely to use VV ECMO (or other medical therapies, such as inhaled vasodilators or diuresis) to unload the right heart, or else to consider severe cardiogenic shock to actually be a contraindication to ECMO (as it suggests a late stage of disease less likely to respond to aggressive care).
There is no obvious timeframe which is “too early,” but patients already at ECMO-ready centers might reasonably wait longer to go on bypass, as it can be done quickly and safely when necessary without requiring interfacility transport.
Cannulation can be done by whomever is skilled and trained, such as cardiac surgery, trauma surgery, trained intensivists, etc.
For VV ECMO, Maryland likes to cannulate the right IJ and right femoral veins, or perhaps the left femoral if needed. They prefer not to cannulate bilateral femorals, and prefers not to use dual-lumen IJ catheters (the Avalon bi-caval catheter), as flow is often not adequate.
Anticoagulate most patients on VV ECMO with heparin to a PTT of 45-55. VA ECMO can go to 60-80. ECMO without anticoagulation can be done if there are bleeding issues, however.
Maryland generally does not titrate FiO2 on the sweep gas. After induction, titrate the sweep; the goal is usually to correct hypercarbia over 6–8 hours, not all at once.
Flow rates at least 4 L/min, unless more is required for hypoxia. RPM <4000 is usually the starting goal.
Prone even while on pump for lung-protective reasons. Chest PT is good too. Prone first for 6-8 hours to ensure tolerance and skin integrity, then do around 4 more sessions of 16 hours each, as a starting goal.
Ventilator settings on VV ECMO can be walked back after induction. Historically they used PEEP 10, PIP 10, RR 10. In heavily consolidated COVID patients, some need more pressure to maintain some degree of recruitment, such as PEEP 15 and PIP 10.
Inhaled vasodilators can be continued or weaned depending on right heart function. Diurese until you develop flow problems (suction events) on the pump, a useful indicator of low intravascular volume.
Have a low threshold to deeply sedate and/or paralyze while on pump to optimize synchrony and facilitate proning. However, Maryland likes to perform “partial paralysis,” with just enough NMB to achieve goals; respiratory rates below 20 or so are considered acceptable.
Early tracheostomy is reasonable, but persistently high requirements for ventilator pressures often pushes it back.
Hypoxemia can occur in VV ECMO patients due to too much flow through the native circulation and shunted lungs. In such cases, beta blockade may actually improve systemic oxygenation.
Plasma free hemoglobin levels may be a useful marker that changing your oxygenator could improve gas exchange.
Decannulate at the bedside when ready, watch them for 24 hours, then boot them out of the ICU; they’re ready.
65%+ of COVID ECMO patients at Maryland are surviving. Data remains slim, but there seems to be decent results in a well-selected population.
In rare cases, patients who neither die nor recover may become candidates for lung transplant.