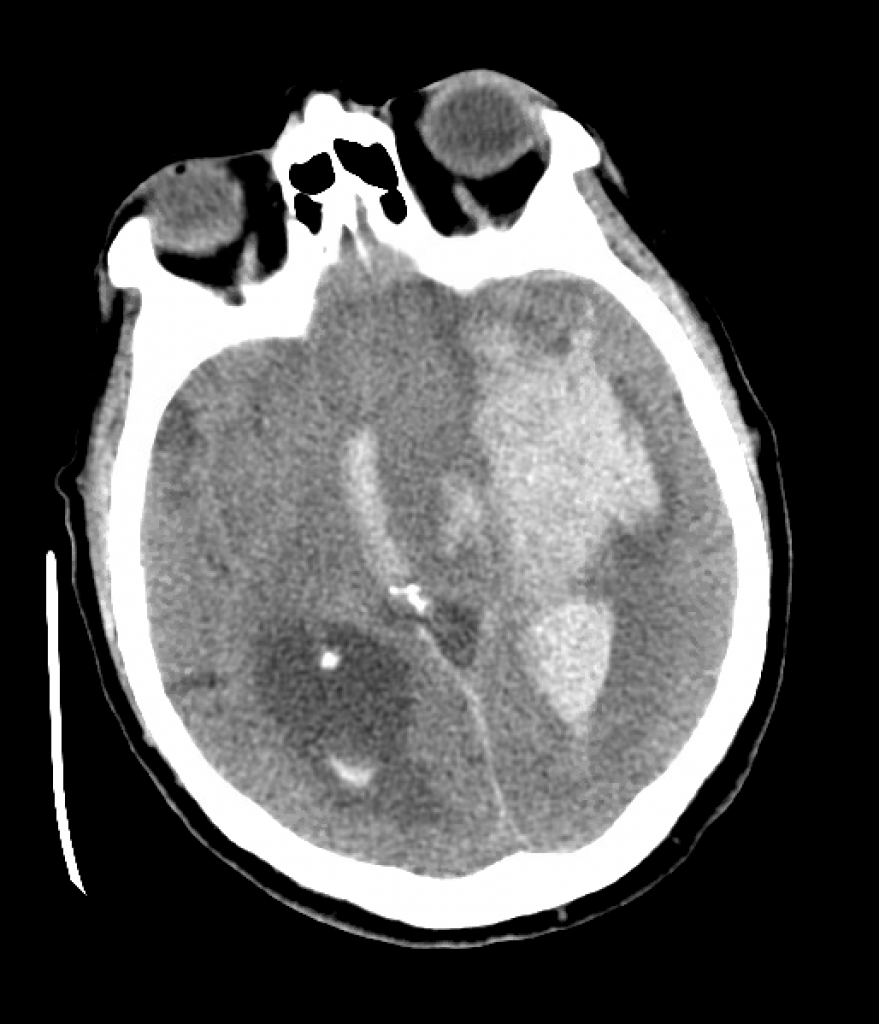
We review a case of massive intraparenchymal hemorrhage progressing to brain death, including the process of brain death testing and declaration, with Dr. Casey Albin (@CaseyAlbin), neurologist and neurointensivist, assistant professor of Neurology and Neurosurgery at Emory and part of the NeuroEmcrit team.
For 20% off the upcoming Resuscitative TEE courses (through July 23, 2022), listen to the show for a promo code for CCS listeners!
Takeaway lessons
In general, in patients with good baseline function, it’s reasonable to be fairly aggressive with initial care, such as placement of intracranial pressure monitors, even if long-term goals of care are unclear—it can always be escalated.
Although ICH score is associated with mortality, the original study allowed withdrawal of care at discretion of the clinicians, so the data may be tainted by self-fulfilling prophecy—withdrawal of care may lead to poor prognosis in some cases, not always the reverse.
Sodium goals are ideally titrated to ICP (with invasive monitoring). In its absence it’s best to target clinical findings, unless you have tools like TCDs or optic nerve sheath ultrasound, or just frequent CT scans. Arbitrary sodium goals are rarely helpful.
There is good evidence for decompressive hemicraniectomy for large MCA infarct IF the patient is young; it is less clear in the elderly. If it’s going to be done, do it early.
If herniation is clear via ICP or imaging, don’t spare sedation for the sake of a neuro exam, unless you’re at the point of stepping back and assessing for long-term futility and possible brain death.
4-5 days into admission is often when families begin to understand the nature of a devastating neurologic injury. In some cases, discussion of futility and brain death may be initiated by families after doing their own research.
The first step is holding sedation and waiting ~5 half-lives for confounding drugs to clear; impaired renal or hepatic clearance should be taken into account here. (Pharmacy may be helpful.) Paralysis should be held and train-of-four can be used to confirm. Drug levels can be used to confirm clearance of opioids, etc if needed.
The law (Uniform Declaration of Death Act) doesn’t always agree with guidelines (while hospital policies may differ even further). The UDDA requires complete brain death, whereas the AAN’s guidelines don’t necessarily require pituitary death (patient need not be in DI), but all do require more than just brainstem death—for example, a locked-in patient would not qualify.
Expect and manage DI, as hypovolemia and hypernatremia may make the patient too unstable to tolerate brain death testing. Consider a vasopressin drip, replace volume, etc.
As the chest wall becomes denervated, it loses elastic recoil, while hypovolemia may cause very hyperdynamic cardiac function. The combination can cause strong chest wall vibrations which may autotrigger the ventilator, often confusing staff and family who believe the patient is breathing spontaneously.
Perform brain death testing in a systematic, scrupulous manner. Print your hospital policy and use it as a formal checklist. You’ll need a bright penlight, a tongue depressor or Yankhauer catheter, a Q-tip or gaue for corneal reflexes, 50 ml x2 of ice-cold water and a syringe with an IV catheter on the tip for cold calorics, and some kind of insufflation catheter or a T-piece for apnea testing.
Pitfalls: remember to test corneals by touching the actual cornea, not the sclera. Cold calorics are performed by irrigating the ear canal and watching for gaze deviation (any deviation shows brainstem activity). Gag reflex must be checked all the way in the back of the oropharynx with vigorous stimulation. Cough and pain responses must also be checked with substantial stimulation. Warn family ahead of time about the possibility of purely reflexive triple flexion.
Consider bringing the family to watch, which helps encourage transparency. Warn them ahead of time that if the test is confirmatory, it will indicate the patient is dead by brain criteria.
You generally want an arterial line for the apnea test, and have vasopressors running and ready to maintain the SBP >100. Put the patient on 100% FiO2 and get a baseline ABG showing normocapnia and a PAO2 >200. (If the patient has a baseline elevated PACO2, follow your local policy.) Oxygenate the patient passively, such as by inserting an insufflation catheter hooked up to oxygen down the ET tube after disconnecting the ventilator. Uncover the patient’s chest and watch for chest rise.
A confirmatory apnea test is one where the PACO2 rises by 20 points, without any clinical signs of breathing; hence the team needs to be in the room, physically observing the patient. An equivocal test is one where the test cannot be completed or the PCO2 fails to adequately rise to confirm adequate levels. Most tests are completed by 10 minutes, but start sending blood gasses earlier than that (e.g. at 6, 8, 10 minutes), as you may need to terminate the test due to instability while waiting for the most recent gas and you’ll want to know if the patient had finished.
Confirmatory/ancillary tests can be done if the clinical and apnea tests cannot be done, or are not completely definitive due to confounding factors. They can include TCDs, nuclear flow studies, or EEG if specialized equipment and readers are available. Catheter-directed 4-vessel cerebral angiography is another option, but CTA/MRA are not. Most of these tests are looking for intracranial circulatory arrest, i.e. lack of blood flow to the brain—dead cells have no metabolic demand and shunt blood away.
Perform brain death testing as soon as clinically appropriate; they only become more unstable.
Resources
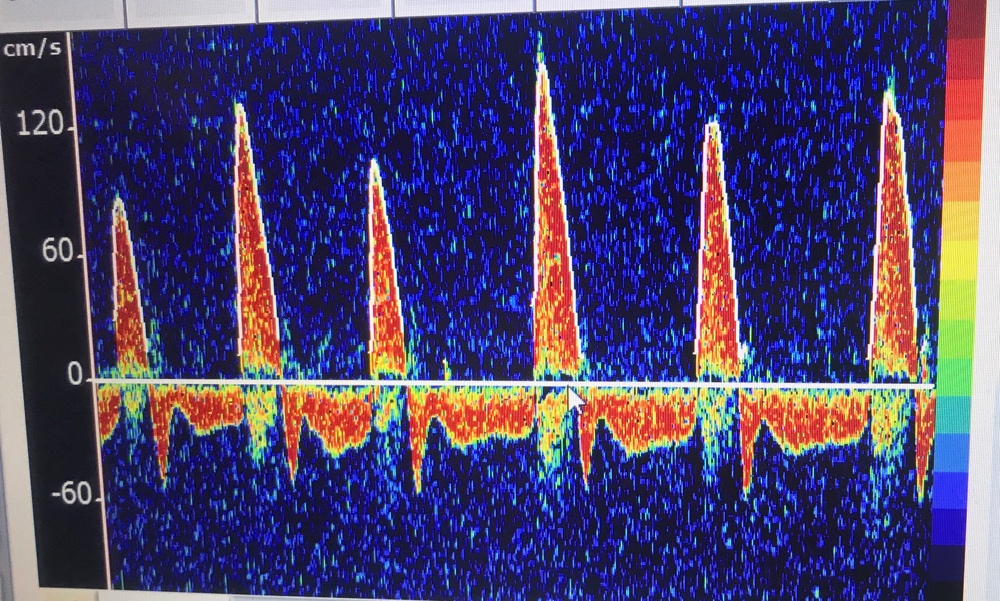
An example of massive ICH with IVH.TCDs in brain death, with sharp systolic spikes and diastolic flow reversal
Brandon and Bryan discuss a practical approach to abdominal compartment syndrome: when to suspect it, confirming the diagnosis with bladder pressure or other monitoring, management, and prognosis.
We discuss the clinical presentation and management of AFE with guests Dr. Stephanie Martin (Twitter: @OBCriticalCare, Instagram: @criticalcareob), medical director for Clinical Concepts in Obstetrics and a Maternal Fetal Medicine specialist in Scottsdale, Arizona with expertise in critical care obstetrics. She is also co-host of the Critical Care Obstetrics podcast. We’re also joined for a patient perspective by Miranda Klassen (@afefoundation), Executive Director of the AFE Foundation, and her husband Bryce Klassen, CCRN, ICU Supervisor at Scripps Memorial Hospital Encinitas.
Takeaway lessons
AFE is poorly understood but is probably caused by exposure of amniotic fluid (skin cells, hair, vernix, etc) to maternal blood, causing a severe inflammatory reaction. Although it may contribute, it is probably not mainly due to obstructive shock, as seen in pulmonary embolism.
AFE is rare. Some clinicians will go an entire career without seeing it. However, it certainly happens and has tremendous consequences when it does.
As a rule, ACLS care is the same for pregnant women. The main exception is that if ROSC is not obtained immediately, you must perform a resuscitative Caesarean section within the first 4 minutes, aiming to have the baby delivered within 5. Without this, the chances of recovering the mother are slim: the gravid uterus interferes with compressions, compresses the IVC, and causes other problems. Achieving this in non-obstetric areas requires a carefully thought-out process. Time must not be wasted transporting the patient elsewhere. The only equipment absolutely required is a scalpel, although this too can be hard to find if you haven’t optimized your process. In short, if you have a pregnant woman in your ICU, figure out now what you’re going to do now if she codes.
Due to the logistical challenges, most of these resuscitative C-sections are actually done in 6-15 minutes. This is not the goal.
During CPR, the gravid uterus should be manually displaced to one side, preferably the left. (It is no longer recommended to tilt the patient laterally, since this interferes with compressions.)
AFE is rare, but with excellent care it is survivable.
Bleeding post C-section is usually not significant. The abdomen can be left open, and can even be used for aortic access to check for the pulse, or occlude the aorta (either manually or by cross-clamp).
A normal fibrinogen level in a pregnant or immediately post-partum female is elevated (often in the ~600s), so a “normal” level should be considered low. Use this to follow DIC. Bleeding and clotting may both occur.
Although pregnant women have a subtle physiologic hemodilution, their normal hemoglobin should not drop below 11, so for our purposes, anemia still denotes anemia.
Resuscitating the immediately post-partum woman should not mean great confusion about safe medications. Use whatever is necessary to save her life. Any impacts on breastmilk can be managed by pumping and either saving or dumping it as appropriate.
A compensated respiratory alkalosis via hyperventilation should be expected during pregnancy (the mother must have a lower PCO2 than the fetus to create a gradient for fetal ventilation). This persists post-partum, so it’s probably appropriate to aim to maintain this by increasing minute ventilation, even although it’s likely not as critical since there’s no longer a fetus to support.
The most important post-partum care after an emergency like this remains supportive critical care. Eventually the mother can be transferred to a post-partum obstetric unit, but these are not high acuity floors (with nurse:patient ratios as high as 8:1) and this needs not be rushed. OB staff can come to the ICU to assist and educate as needed.
If you have a suspected AFE, call the AFE Foundation 24/7 (307-363-2337) for advice and to coordinate collection of specimens, which must be done promptly and is badly needed to improve our understanding of this disease.
References
Amniotic fluid embolism: principles of early clinical management. Pacheco, Luis D, Klassen, M., et. al. American Journal of Obstetrics & Gynecology.
Society for Maternal-Fetal Medicine (SMFM). Pacheco LD, Saade G, et al. Amniotic fluid embolism: diagnosis and management. Am J Obstet Gynecol 2016; 215:B16.
Stafford, IA, Moaddab, A, Dildy, GA (2019) Evaluation of proposed criteria for research reporting of amniotic fluid embolism. AJOG, 220, 285-287.
Combs CA, Montgomery DM, Toner LE, Dildy GA, Patient Safety and Quality Committee, Society for Maternal-Fetal Medicine, Society for Maternal-Fetal Medicine Special Statement: Checklist for initial management of amniotic fluid embolism, American Journal of Obstetrics
Amniotic fluid embolism: Pathophysiology from the perspective of pathology. Tamura N, Farhana M, Oda T, Itoh H, Kanayama N. J Obstet Gynaecol Res. 2017;43(4):627. Epub 2017 Feb 11.
Kiranpreet, K., Bhardwaj, M, Kumar, P., Singhai, S., Singh, T., & Hooda, S. (2016). Amniotic fluid embolism. J Anesthesiol Clin Pharmacol, 32(2), 153-159.
Zelop CM, Einav S, Mhyre JM, Lipman SS, Arafeh J, Shaw RE, Edelson DP, Jeejeebhoy FM; American Heart Association’s Get With the Guidelines-Resuscitation Investigators. Characteristics and outcomes of maternal cardiac arrest: A descriptive analysis of Get with the guidelines data. Resuscitation. 2018 Nov;132:17-20. doi: 10.1016/j.resuscitation.2018.08.029. Epub 2018 Aug 28. PMID: 30170022.
A look at rehabilitation and mobility in the critically ill, from the perspective of our skilled therapists—with Heidi Engel, PT, DPT of UC San Francisco, long-term provider of acute care therapy, researcher in ICU rehabilitation, and founding member of the SCCM’s ICU Liberation program.
Takeaway lessons
Tolerance of pressure support ventilation is often a good marker that a patient is ready to start meaningful PT. Before that, the harm may exceed the benefit, unless there’s a specific reason why activity may help move them along, such as attenuating delirium and agitation and improving tolerance of the ET tube.
The most common complaints and stressors of ICU patients are: feeling thirsty, feeling traumatized and afraid, the inability to communicate, and feeling “air hungry” due to the strange mechanics of mechanical ventilation and other respiratory modalities.
In many cases, rehab will require convincing patients to get over an initial hump. Breathing, strength, and discomfort may initially be a challenge but will improve with activity.
You may need to choose priorities: do you want to push vent liberation or mobility today?
Bring the light during daytime hours to improve the circadian rhythm, but direct fluorescent lights are harsh and can encourage closed eyes. Natural, indirect light is better.
Although PT and OT have complementary roles, they will sometimes try to see patients together, which can have downsides by underemphasizing the unique aspects of each role, reducing total rehab time, and relegating one skilled therapist to acting as merely a set of hands.
The presence of any sedation, even “gentle” agents like precedex, creates an obstacle to effective PT.
Getting patients up to a chair helps with agorophobia by changing their perspective from their tiny bed-shaped home.
Heidi’s rehab process
Check the RASS and CAM-ICU scores
Explain to patient the importance of the endotracheal tube and not touching it. Bring all equipment to the side of the bed with the ventilator.
Perform some gastroc/hamstring stretching to initiate mobility and help wake the patient up
Ask them to follow commands, such as: push! Can they follow? Do the vent and vitals remain okay?
Sit them up at edge of bed, arrange equipment. Observe head control, trunk control, breathing, vitals, orthostasis, etc.
bring a big mobility device, see if they can stand.
While they’re up, use the opportunity to clean the linen, wash their face, comb their hair, clean their posterior.
COVID is making it harder, often just for practical reasons: PPE limiting mobility, noise from filters and masks, families not present, weird autonomic and orthostatic issues… all far more time consuming. However, they do get better and many times do very well, sometimes even recovering faster than similar non-COVID patients. Omicron has not been as bad.
Dedicated therapy teams for the ICU add cost, but cost analyses have shown the benefit (in terms of reducing length of stay and other expenses) to actually result in net cost savings.
In-bed, non-weight-bearing activities such as passive range of movement exercise is perhaps better than nothing, but is nowhere near as useful as weightbearing activity out of bed, and has not shown the same clinical benefits in the literature. Every day of out-of-bed activity may pay back several fewer days of rehab down the road.
Brandon and Bryan reflect on the qualities that define good and bad ICU nurses, the challenges they face, and how APPs and physicians can enable them to be their best.
Why an assumption in your training should be to call for assistance, but expect it will never arrive. Plan to manage problems yourself. Let help surprise you—otherwise hope becomes your plan.